

Lesion Analysis of 18F-Metafluorobenzylguanidine PET Imaging in Neuroblastoma
- PMID: 40908121
- PMCID: PMC12487752
- DOI: 10.2967/jnumed.125.269833
Lesion Analysis of 18F-Metafluorobenzylguanidine PET Imaging in Neuroblastoma
Abstract
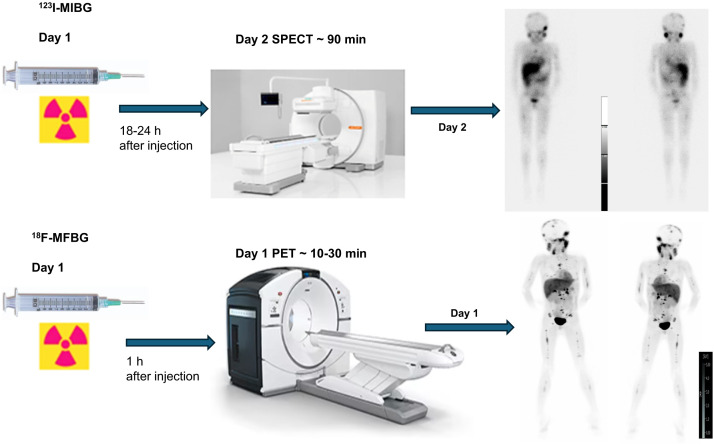
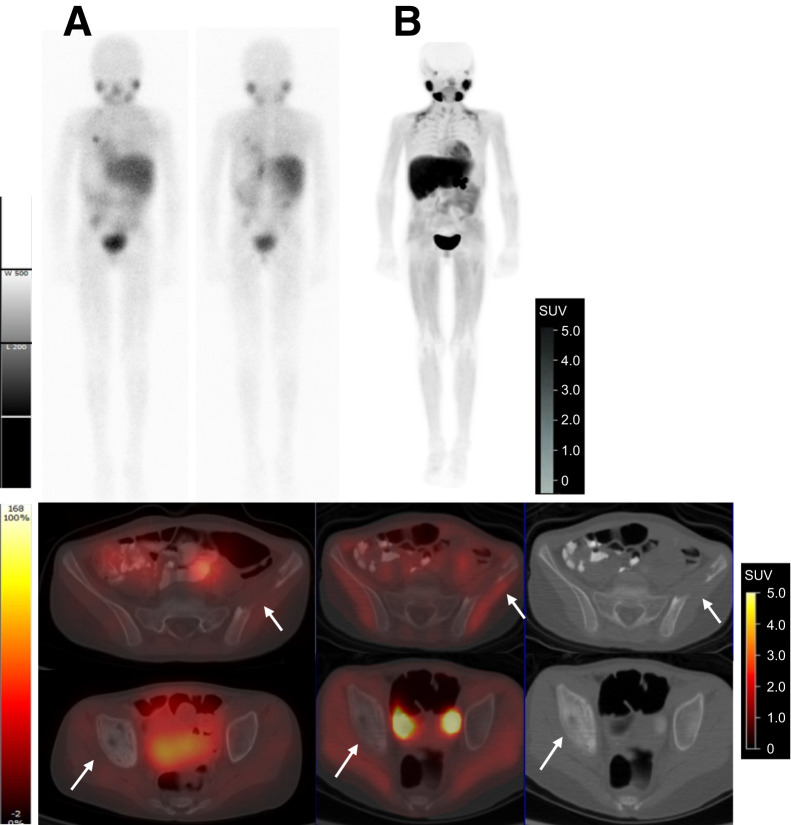
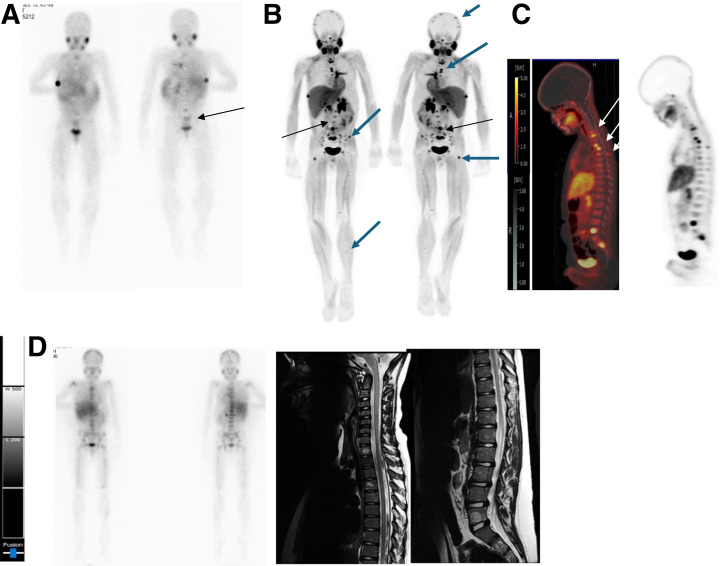
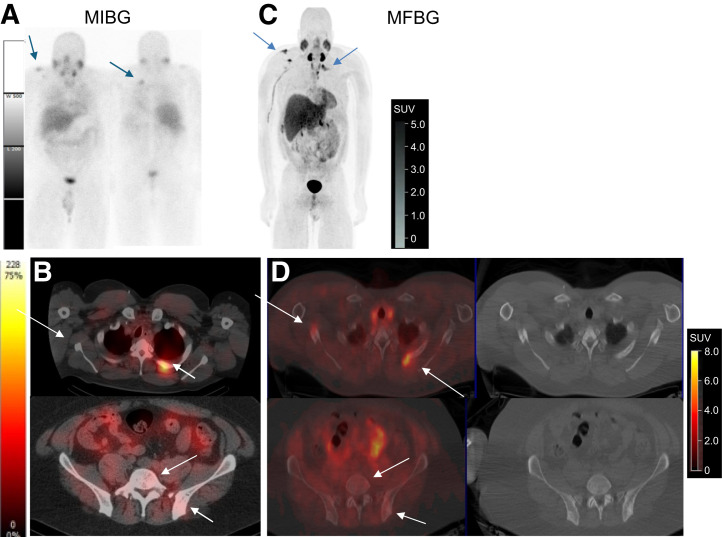
A PET analog of metaiodobenzylguanidine (MIBG)-18F-metafluorobenzylguanidine (18F-MFBG)-allows for rapid same-day imaging. We previously reported on the safety and feasibility of 18F-MFBG PET imaging in patients with neuroendocrine tumors. We now report a comprehensive analysis of lesion detection with 18F-MFBG imaging in patients with neuroblastoma compared with 123I-MIBG imaging. Methods: We analyzed concurrent 18F-MFBG and 123I-MIBG scans in 37 patients (40 paired scans). Patients with relapsed or refractory neuroblastoma were included. Patients received 74.11-465.83 MBq (2.0-12.6 mCi) of 18F-MFBG intravenously, followed by imaging 60 min after injection. All patients had an 123I-MIBG scan within 4 wk of 18F-MFBG imaging without any intervening therapy. 123I-MIBG scans included whole-body planar and SPECT/CT of the chest, abdomen, and pelvis. All detected lesions were noted for each modality. 123I-MIBG and 18F-MFBG findings were evaluated for concordance and discordance. Modified Curie scores were assigned to both 123I-MIBG scans, equivalent scores were ascertained for 18F-MFBG imaging, and scores were then compared. Results: All patients with a positive 123I-MIBG scan had positive 18F-MFBG imaging. In 2 patients, both 123I-MIBG and 18F-MFBG scans were negative. In 1 patient, the 18F-MFBG scan was positive, whereas the 123I-MIBG scan was negative. In 30 of 40 scans, 18F-MFBG showed more sites than did 123I-MIBG. Overall, more lesions were noted on the 18F-MFBG scans (mean, 18; range 0-61) compared with the 123I-MIBG scans (mean, 12; range, 0-44), and 455 lesions were concordant. The Curie score for 18F-MFBG was higher, with an average of 11 (range, 0-25) compared with 8 for 123I-MIBG (range, 0-22). Of the 273 18F-MFBG-positive/123I-MIBG-negative lesions, follow-up clinical and imaging assessment was available for 234 lesions in 30 patients, and 100% of these were confirmed true-positive. Conclusion: 18F-MFBG PET offers faster imaging and superior detection compared with 123I-MIBG imaging. 18F-MFBG had high concordance with 123I-MIBG at the patient level and showed more lesions in most patients. 18F-MFBG is an attractive alternative to 123I-MIBG.
Keywords: 123I-MIBG; 18F-MFBG; dosimetry; neuroblastoma; neuroendocrine.
© 2025 by the Society of Nuclear Medicine and Molecular Imaging.
Figures

References
-
- Brisse HJ, McCarville MB, Granata C, et al.; International Neuroblastoma Risk Group Project. Guidelines for imaging and staging of neuroblastic tumors: consensus report from the International Neuroblastoma Risk Group Project. Radiology. 2011;261:243–257. - PubMed
-
- Jacobson AF, Deng H, Lombard J, Lessig HJ, Black RR. 123I-meta-iodobenzylguanidine scintigraphy for the detection of neuroblastoma and pheochromocytoma: results of a meta-analysis. J Clin Endocrinol Metab. 2010;95:2596–2606. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical