

Late-Onset Bone Metastasis 46 Years After Initial Surgery for Pheochromocytoma: A Case Report
- PMID: 40909300
- PMCID: PMC12408166
- DOI: 10.1002/iju5.70086
Late-Onset Bone Metastasis 46 Years After Initial Surgery for Pheochromocytoma: A Case Report
Abstract
Introduction: Pheochromocytoma is a rare catecholamine-producing tumor with metastatic potential. Recurrence after more than 40 years is exceptionally rare.
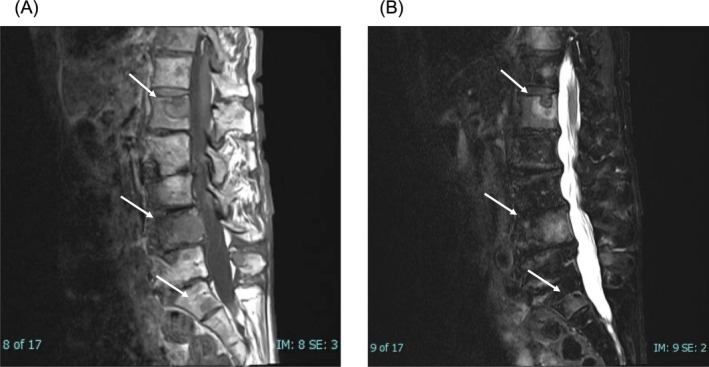
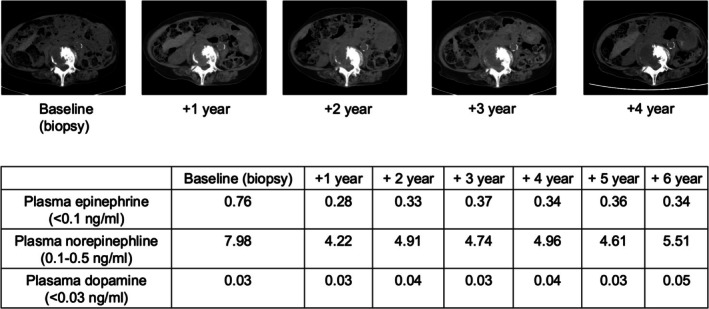
Case presentation: During evaluation for ischemic colitis, a 71-year-old woman was found to have multiple bone metastases, possibly linked to catecholamine excess. She had undergone left adrenalectomy for pheochromocytoma at age 25. Bone biopsy confirmed metastatic pheochromocytoma, and immunohistochemical findings were similar to the original tumor. Urinary metanephrine and normetanephrine were markedly elevated. She declined systemic therapy and has remained clinically stable for 6 years, with her blood pressure well controlled on doxazosin.
Conclusion: This case illustrates a recurrence 46 years after adrenalectomy, potentially representing the longest reported interval to date. It highlights the silent and indolent nature of some metastatic pheochromocytomas and underscores the necessity of lifelong follow-up. The patient's stable course also emphasizes the clinical heterogeneity of metastatic pheochromocytoma and supports the need for individualized follow-up and treatment strategies.
Keywords: bone metastasis; late recurrence; pheochromocytoma.
© 2025 The Author(s). IJU Case Reports published by John Wiley & Sons Australia, Ltd on behalf of Japanese Urological Association.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
LinkOut - more resources
Full Text Sources