

Isolated spinal aneurysms with spontaneous regression
- PMID: 40920243
- PMCID: PMC12417233
- DOI: 10.1007/s10143-025-03768-8
Isolated spinal aneurysms with spontaneous regression
Abstract
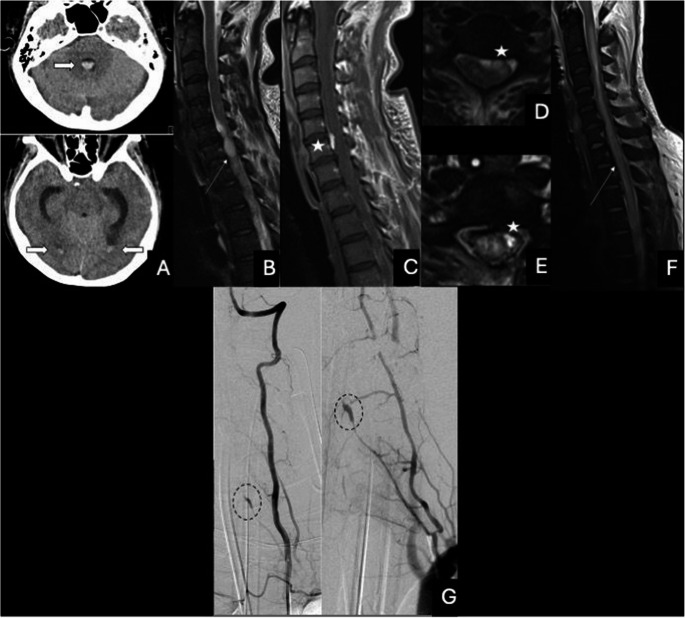
Purpose: To share our clinical experience with conservative management of isolated spinal arterial aneurysms (ISAs) and to identify clinical scenarios where conservative management may be appropriate, in the context of a literature review.
Methods: We performed a retrospective review of spinal angiograms from two German neuroradiology centers and conducted a systematic literature review of reported ISA cases. We analyzed demographics, clinical presentation, imaging findings, treatments, and outcomes.
Results: We identified seven patients (mean age 48; 4 women) with nine ISAs, eight of which were managed conservatively. Five of them had excellent short-term outcomes, and spontaneous regression was documented in four cases. With our cases, 208 ISAs have been reported in the literature in 164 patients (mean age 51; 52% female). They most commonly present with subarachnoid hemorrhage (90%) and back pain (69%). Most are located in the thoracic (51%) or cervical spine (40%) and involve the anterior spinal circulation (63%). They may be treated by surgical intervention (47%) or conservatively (37%), less commonly by endovascular therapy (16%). 78% of patients have favorable outcomes (mRS 0-3), similar across all treatment approaches. In 52% of conservatively managed cases, spontaneous regression was documented by imaging. Clinical deterioration was primarily associated with respiratory complications and spinal cord infarction, with a documented rebleeding rate of 8% and a mortality rate of 12%.
Conclusions: ISAs are a rare and potentially underrecognized cause of cerebral and spinal subarachnoid hemorrhage. In select cases, particularly small ISAs of the anterior spinal or a radiculomedullary artery and with transient neurological symptoms, conservative management appears to be a reasonable approach, supported by increasing evidence of the possibility of spontaneous regression.
Keywords: Spinal aneurysm; Spinal angiography; Spinal hemorrhage; Subarachnoid hemorrhage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: was waived by the local Ethics Committee in view of the retrospective nature of the study and all the procedures being performed were part of the routine care. Consent to participate: was obtained from all patients for scientific use of imaging data without identifying factors. Competing interests: The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
