

Two-year outcomes of quantitative flow ratio-based physiology-guided percutaneous coronary intervention in patients with low-risk acute coronary syndrome: a prespecified secondary analysis of FAVOR III China
- PMID: 40926902
- PMCID: PMC12414827
- DOI: 10.1016/j.eclinm.2025.103461
Two-year outcomes of quantitative flow ratio-based physiology-guided percutaneous coronary intervention in patients with low-risk acute coronary syndrome: a prespecified secondary analysis of FAVOR III China
Abstract
Background: The benefits of physiology-guided management in acute coronary syndrome (ACS) remain inconclusive due to limited evidence. In our FAVOR III China trial, a quantitative flow ratio (QFR)-based physiology-guided strategy versus standard angiography guidance improved the 1-year primary outcome among participants with coronary artery disease (CAD). We aimed to investigate, in a prespecified analysis, the outcomes of QFR-based physiological guidance in the FAVOR III China participants with low-risk ACS.
Methods: This pre-specified secondary analysis included patients diagnosed with low-risk ACS who were enrolled in the FAVOR III China trial. The trial was a prospective, randomised study that assigned 3825 CAD patients to receive QFR-guided or angiography-guided percutaneous coronary intervention (PCI) at 26 hospitals in China between December, 2018 and January, 2020. The primary outcome of interest for this study was major adverse cardiac events (MACE), defined as a composite of all-cause death, myocardial infarction, and ischaemia-driven revascularisation, at 1-year (primary outcome of FAVOR III China) and 2-year follow-up. Secondary outcomes included PCI strategy change and the procedural characteristics. FAVOR III China is registered with ClinicalTrials.gov, NCT03656848.
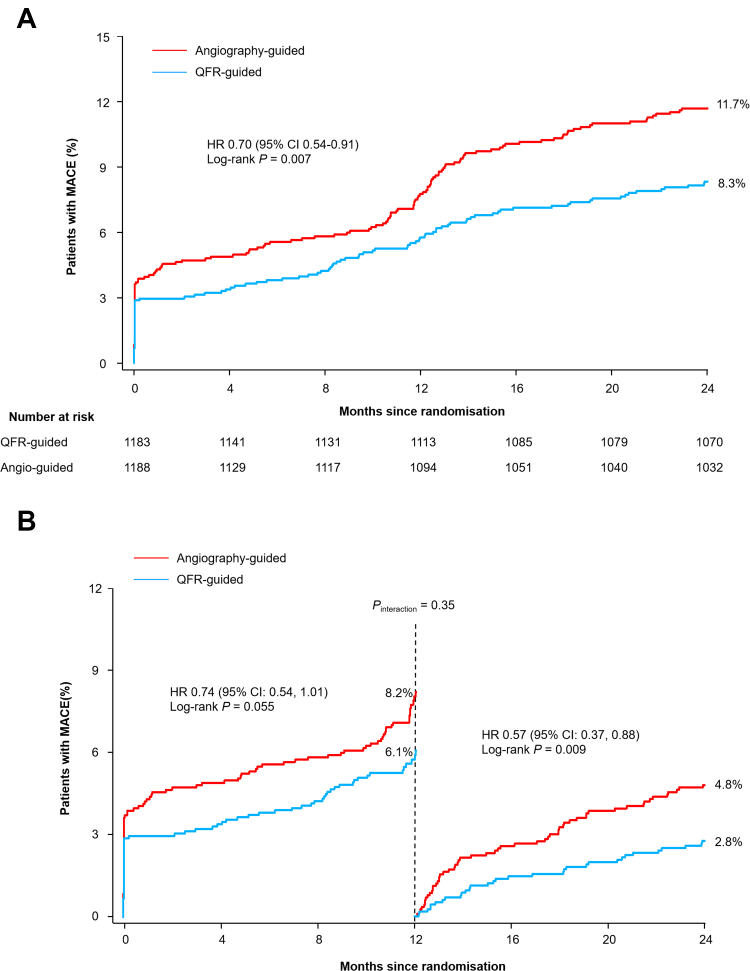
Findings: Of the 2371 participants with low-risk ACS (93.7% unstable angina and 6.3% non-ST elevation myocardial infarction [NSTEMI]) in the FAVOR III China trial, the QFR-guided strategy changed the original intended treatment plan in 23.6% of the low-risk ACS patients, resulting in more PCI deferrals (19.0% vs 3.8%; P < 0.001), less stenting (1.5 ± 1.1 vs 1.6 ± 1.0 per participant; P = 0.034), and shorter fluoroscopy time (13.7 ± 7.7 min vs 14.6 ± 7.1 min; P = 0.01) compared with the angiography-guided strategy. During follow-up, there was some evidence that the QFR guided strategy is superior to the angiography-guided approach at reducing the risk of MACE at 1-year follow-up (6.1% vs 8.2%; HR, 0.74; 95% CI, 0.54-1.01, P = 0.055), with a significant risk reduction at 2-year follow-up (8.3% vs 11.7%; HR, 0.70; 95% CI, 0.54-0.91, P = 0.009). The landmark analysis indicated consistent patterns both before and after 1 year (P interaction = 0.35).
Interpretation: Our findings favoured the superiority of QFR-guided lesion selection strategy over standard angiography guidance in reducing long-term MACE for the low-risk ACS population. The benefits associated with QFR need to be confirmed by future studies with extended follow-up.
Funding: The National High Level Hospital Clinical Research Funding, the Capital's Funds for Health Improvement and Research, the Chinese Academy of Medical Sciences, the Noncommunicable Chronic Diseases National Science and Technology Major Project, Shanghai Municipal Health Commission "Top Priority Research Centre", and Shanghai Shenkang Hospital Development Centre.
Keywords: Acute coronary syndrome; Fractional flow reserve; Physiological guidance; Quantitative flow ratio; Revascularisation strategy.
© 2025 The Author(s).
Conflict of interest statement
Dr Tu is the co-founder of Pulse Medical, reports grants and consultancy from Pulse Medical. Dr Kirtane reports grants and travel or meal reimbursements from Medtronic, Abbott Vascular/St Jude, Boston Scientific, Abiomed, Siemens/Corindus, Philips/Spectranetics, ReCor Medical, and Cardiovascular Systems; grants from CathWorks; travel or meal reimbursements from Chiesi, Opsens, Zoll, and Regeneron; and consulting fees from IMDS, outside the submitted work. All other authors report no competing interests.
Figures


References
-
- Lawton J.S., Tamis-Holland J.E., Bangalore S., et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21–e129. - PubMed
-
- Pijls N.H., van Schaardenburgh P., Manoharan G., et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol. 2007;49(21):2105–2111. - PubMed
-
- van Nunen L.X., Zimmermann F.M., Tonino P.A., et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet. 2015;386(10006):1853–1860. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
