

Efficacy and Safety of Aldosterone Synthase Inhibitors for Resistant Hypertension: A Systematic Review and Meta-Analysis
- PMID: 40927087
- PMCID: PMC12415759
- DOI: 10.31083/RCM39555
Efficacy and Safety of Aldosterone Synthase Inhibitors for Resistant Hypertension: A Systematic Review and Meta-Analysis
Abstract
Background: Compared to patients with controllable hypertension, those with resistant hypertension (RH) have a higher incidence of cardiovascular complications, including stroke, left ventricular hypertrophy, and congestive heart failure. Therefore, an urgent need exists for improved management and control, along with more effective medications. Aldosterone synthase inhibitors (ASIs) are newly emerging drugs that have gradually attracted an increasing amount of attention.
Methods: The Cochrane Library, PubMed, Embase, and ClinicalTrials.gov databases were systematically searched to identify all literature on ASIs and resistant hypertension. Additionally, the reference lists of the included articles were manually searched. The quality of the identified studies was assessed using the Cochrane Bias Risk Tool.
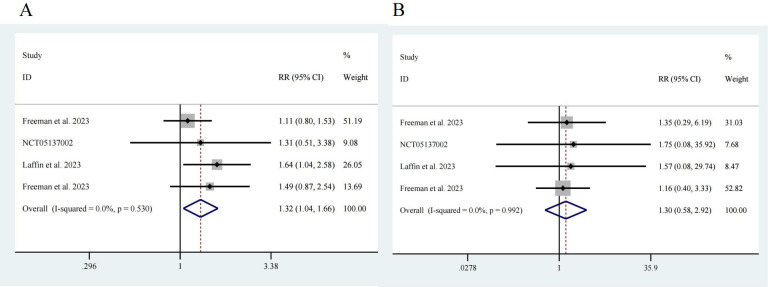
Results: This study comprised four randomized controlled trials (RCTs), involving 776 participants. Different doses of ASIs were used, with treatment durations ranging from 7 to 12 weeks. The selected study population included individuals with resistant hypertension and healthy adults. Systolic blood pressure (SBP) had a pooled effect size of standardized mean difference (SMD) = -0.24, with a 95% confidence interval (CI) of [-0.46, -0.03], indicating a statistically significant difference (p = 0.026); however, diastolic blood pressure (DBP) had a pooled effect size of SMD = -0.13, with a 95% CI of [-0.40, 0.15], indicating no significant difference (p = 0.359). Similarly, subgroup analyses yielded comparable results. Notably, the risk of adverse events in the ASI group was greater than that in the control group, with a risk ratio of 1.32 and a 95% CI of [1.04, 1.66], indicating a significant difference (p = 0.02). There was no statistically significant difference in severe adverse events between the treatment group and the control group (p = 0.532).
Conclusions: ASIs have shown benefits in controlling SBP in patients with resistant hypertension, although their effects on DBP appear to be limited. Given the observation period of only 12 weeks, the potential for increased adverse event risks with their use warrants further attention. Considering the relatively small number of trials included and the limited sample size in this study, future research should focus on expanding the sample size and extending the follow-up duration to more precisely define the clinical role and value of ASIs. Additionally, further investigation into the underlying mechanisms of action of these inhibitors is necessary to provide theoretical support for optimizing treatment strategies for resistant hypertension and related conditions.
Keywords: aldosterone synthase; inhibitor; resistant hypertension; risk.
Copyright: © 2025 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- An J, Kurella Tamura M, Odden MC, Ni L, Thomas IC, Montez-Rath ME, et al. Prevalence of Apparent Treatment-Resistant Hypertension in Chronic Kidney Disease in Two Large US Health Care Systems. Clinical Journal of the American Society of Nephrology: CJASN . 2022;17:1457–1466. doi: 10.2215/CJN.04110422. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
