

Utility of SPECT/CT in Non-Traumatic Osteonecrosis: Revisited with New Insights from a Prospective Diagnostic Study
- PMID: 40927156
- PMCID: PMC12416583
- DOI: 10.4103/ijnm.ijnm_13_25
Utility of SPECT/CT in Non-Traumatic Osteonecrosis: Revisited with New Insights from a Prospective Diagnostic Study
Abstract
Objectives: Bone scintigraphy is a sensitive imaging method to evaluate patients with suspected osteonecrosis. We assessed the diagnostic performance of combined bone single-photon emission computed tomography/computed tomography (SPECT/CT) (CBS) in patients with known rheumatic disease or other connective tissue disorders and clinical suspicion of osteonecrosis compared to magnetic resonance imaging (MRI).
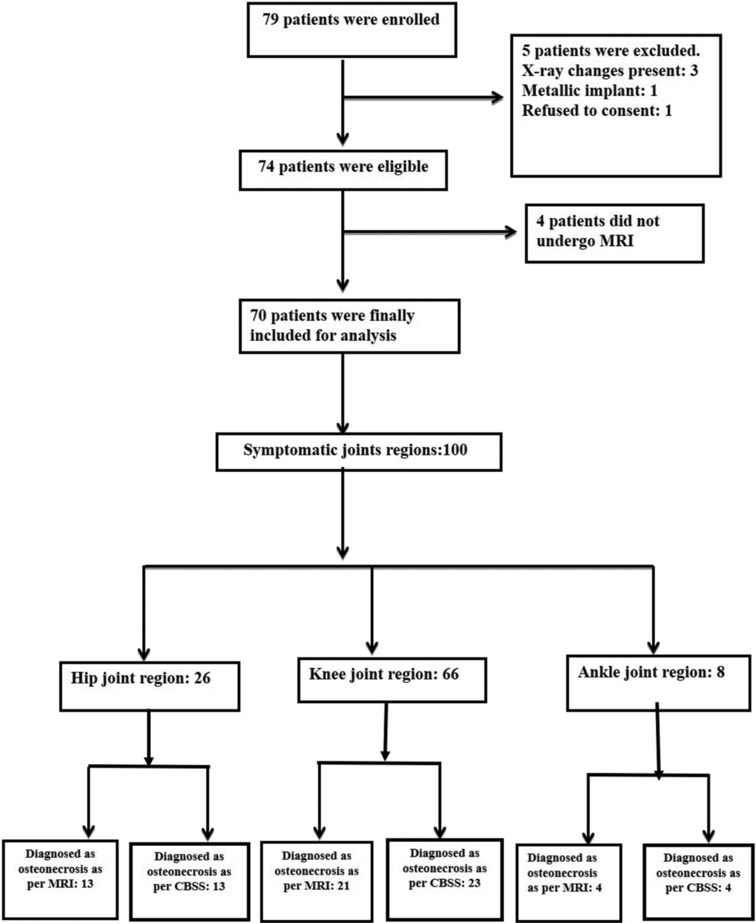
Methods: This prospective diagnostic accuracy study included 70 patients with clinical suspicion of osteonecrosis in any bone who underwent a planar triple-phase bone scan along with a regional SPECT/CT (CBS) and regional MRI. MRI was considered the standard for diagnosing the sensitivity, specificity, predictive values, and accuracy of CBS. Cohen's kappa statistic of the agreement was also calculated.
Results: The distribution of the patients based on the joint regions suspected to have osteonecrosis is as follows: 21 hip, 43 knee, and six ankle. MRI detected osteonecrosis in 30/70 patients. CBS had a sensitivity of 100% (30/70 were detected) and a specificity of 97% (2/40 were false positive). Overall, there was good agreement between the two scans regarding the diagnosis of osteonecrosis (Cohen's kappa statistic = 0.94). In addition to the suspected sites, CBS detected osteonecrosis in 19 additional asymptomatic sites in 13 patients.
Conclusion: The study has demonstrated that CBS, which includes whole-body imaging and SPECT/CT, is highly sensitive in detecting osteonecrosis with accuracy comparable to regional MRI. Its inherent whole-body imaging technique enabled the detection of multifocal osteonecrosis. It can be used as an early investigating modality after routine plain radiography to establish the diagnosis.
Keywords: Magnetic resonance imaging; nontraumatic osteonecrosis; rheumatic and autoimmune diseases; single-photon emission computed tomography/computed tomography; triple-phase bone scan.
Copyright: © 2025 Indian Journal of Nuclear Medicine.
Conflict of interest statement
There are no conflicts of interest.
Figures





References
-
- Mankin HJ. Nontraumatic necrosis of bone (osteonecrosis) N Engl J Med. 1992;326:1473–9. - PubMed
-
- Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME. Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum. 2002;32:94–124. - PubMed
-
- Weiner ES, Abeles M. Aseptic necrosis and glucocorticosteroids in systemic lupus erythematosus: A reevaluation. J Rheumatol. 1989;16:604–8. - PubMed
-
- Yang Y, Kumar S, Lim LS, Silverman ED, Levy DM. Risk factors for symptomatic avascular necrosis in childhood-onset systemic lupus erythematosus. J Rheumatol. 2015;42:2304–9. - PubMed
LinkOut - more resources
Full Text Sources