

Circulating Tumor DNA as a Prognostic Biomarker for Selecting Participants to Early Phase Clinical Trials
- PMID: 40927309
- PMCID: PMC12416488
- DOI: 10.36401/JIPO-25-11
Circulating Tumor DNA as a Prognostic Biomarker for Selecting Participants to Early Phase Clinical Trials
Abstract
Introduction: Patients with advanced solid tumors may be considered for early phase clinical trials investigating the safety, tolerability, and dosing of experimental therapies. Optimizing participant selection is critical to maximize clinical benefit and meet trial endpoints with fewer participants. One in six participants does not meet routine life expectancy requirements (>3 months), highlighting the need for improved prognostication. Variant allele frequency (VAF) in circulating tumor DNA (ctDNA) correlates with overall survival (OS) in advanced solid tumors. We aimed to derive an optimal VAF threshold as a prognostic biomarker to enhance participant selection.
Methods: ctDNA testing was performed as part of the TARGET (NIHR Clinical Research Network CPMS ID 39172) and TARGET National (NCT04723316) prospective cohort studies, in patients with advanced solid tumors referred for early phase clinical trials. Maximum (maxVAF) and mean VAF (meanVAF) were compared in their association with OS and ability to delineate favorable and poor outcomes at set threshold points using hazard ratios (HRs). Optimal thresholds of VAF were explored using receiver operating characteristic curve analysis to predict 3-month landmark OS. Univariable and multivariable analysis was performed to determine whether VAF was an independent prognostic marker.
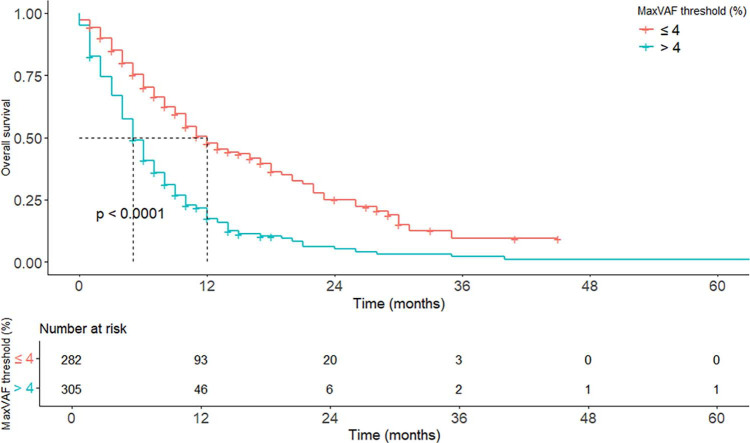
Results: Of 631 patients, 587 had evaluable ctDNA results. MeanVAF and maxVAF exhibited similar correlation with OS (rs = -0.32 vs -0.35, respectively) and similar prognostic utility at matched threshold points. A maxVAF value of 4% was selected as optimal for prognostic subgrouping (area under curve 0.77). OS was 5.9 versus 12.1 months (p < 0.0001) for patients with more than 4% and 4% or less maxVAF, respectively. Multivariable analysis confirmed more than 4% maxVAF as independently associated with reduced 3-month landmark OS (HR 2.17 [1.76-2.70], p < 0.001).
Conclusion: VAF is an independent prognostic marker in patients with advanced solid tumors, with 4% maxVAF deemed optimal for delineating favorable and poorer prognostic subgroups in this patient cohort. Further validation and integration into existing prognostic scores are warranted.
Keywords: advanced solid tumors; circulating tumor DNA; early phase clinical trials; prognostic biomarker; variant allele frequency.
Conflict of interest statement
Conflicts of Interest: Alastair Greystoke, Louise Carter, Fiona Thistlethwaite, Natalie Cook, Donna M. Graham, and Matthew G. Krebs have potential conflicts of interest that are disclosed at the end of this article. The remaining authors have no disclosures.The following authors have disclosed potential conflicts of interest. Alastair Greystoke: consultant and speaker fees from AstraZeneca, Amgen, Boehringer–Ingelheim, Bristol–Myers Squibb (BMS), Janssen/J&J, MSD, Novartis, Pfizer, Lilly, Takeda, and Roche; institutional research funding from AstraZeneca; clinical lead for Cancer North East England Hull, and Yorkshire Genomic Laboratory Hub; and a member of the National Test Directory Evaluation Working Group. Louise Carter: consultant role/attended advisory boards for Bicycle Therapeutics; and institutional funding from Sierra Oncology, Athenex, Takeda, CellCentric, CytomX Therapeutics, Eli Lilly, Boehringer Ingelheim, Bicycle Therapeutics, Lupin Pharmaceuticals, Repare Therapeutics, ADC Therapeutics, Merck Serono, Moma Therapeutics, Loxo Oncology, and Nurix Therapeutics. Fiona Thistlethwaite: institutional research funding from GSK, Pfizer, GenMab, CytomX, Incyte, Janssen, Adaptimmune, BMS, Immunocore, Achilles Ltd, Crescendo, Oxford Vacmedix, RS Oncology LLC, Roche, AstraZeneca, Kymab Ltd/Sanofi, Chugai, T–Knife, Novalgen, Iovance, Nucana, Biontech, Moderna, Zymeworks, Seagen, and Grey Wolf Therapeutics; consultant roles for Guidepoint; honoraria from AstraZeneca; advisory board participation for CytomX, Grey Wolf Therapeutics, Oncobayes, Waypoint, T–Knife Therapeutics, Immatics, and Scenic Biotech; travel and meeting support from ESMO; unpaid leadership roles as a funding committee member for MRCP DPFS and GAP; scientific advisory roles for Sarcoma UK and Target Ovarian Cancer;and serves as a scientific committee member for ESMO Congress, TAT Congress, and ESMO IO. Natalie Cook: consulting fees from Roche Pharmaceuticals, Servier, and REDX Pharmaceuticals; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Roche Pharmaceuticals; support for attending meetings and/or travel from Roche Pharmaceuticals; research funding to research team from AstraZeneca, Orion, F. Hoffmann–La Roche Ltd, Taiho, Novartis, Starpharma, Bayer, Eisai, UCB, RedX Pharmaceuticals, LOXO–oncology, Avacta, Boehringer Ingelheim, Merck, and Tarveda Therapeutics; and participation in data safety monitoring board or advisory board at Roche Pharmaceuticals and Cancer Research UK. Donna M. Graham: honoraria from the Cancer Drug Development Forum; consultant roles for Clinigen Group; institutional research funding from Taiho Pharmaceutical, Merck Sharp & Dohme, Debiopharm Group, Incyte, Carrick Therapeutics, Bayer, AstraZeneca, Bristol–Myers Squibb, Synthon, BerGenBio, Genmab, Takeda, Roche, CytomX Therapeutics, Eisai, Janssen, Athenex, Novartis, Octimet, Redx Pharma, Sierra Oncology, 3–V Biosciences, Actuate Therapeutics, Blueprint Medicines, Boehringer Ingelheim, Ignyta, Macrogenics, Millenium Pharmaceuticals, Orion, Adaptimmune, GlaxoSmithKline, and MedImmune; and travel and accommodation support from Novartis. Matthew G. Krebs: advisory boards or consultancy roles for Astellas, Bayer, Guardant Health, Janssen, Roche, and Seattle Genetics; acts as scientific advisory board member for Zai Therapeutics; travel support from BerGenBio, BMS, Janssen, Roche, and Zai Lab; institutional research funding from Novartis and Rochel; and speaker fees from BMS, Eisai, Janssen, and Roche.
Figures


References
-
- Ortega–Franco A, Darlington E, Greystoke A, Krebs MG. TARGET National: a UK–wide liquid–based molecular profiling programme: on behalf of the TARGET National Consortium. Clin Oncol. 2023;35:33–37. - PubMed
-
- Park S, Olsen S, Ku BM, et al. High concordance of actionable genomic alterations identified between circulating tumor DNA-based and tissue-based next-generation sequencing testing in advanced non–small cell lung cancer: the Korean Lung Liquid Versus Invasive Biopsy Program. Cancer. 2021;127:3019–3028. - PubMed
-
- List of cleared or approved companion diagnostic devices (in vitro and imaging tools) . Food and Drug Administration. Accessed June 23, 2025. www.fda.gov/medical-devices/in-vitro-diagnostics/list-cleared-or-approve...
LinkOut - more resources
Full Text Sources