

ABO blood group antigens influence host-microbe interactions and risk of early spontaneous preterm birth
- PMID: 40931094
- PMCID: PMC12423329
- DOI: 10.1038/s41522-025-00783-x
ABO blood group antigens influence host-microbe interactions and risk of early spontaneous preterm birth
Abstract
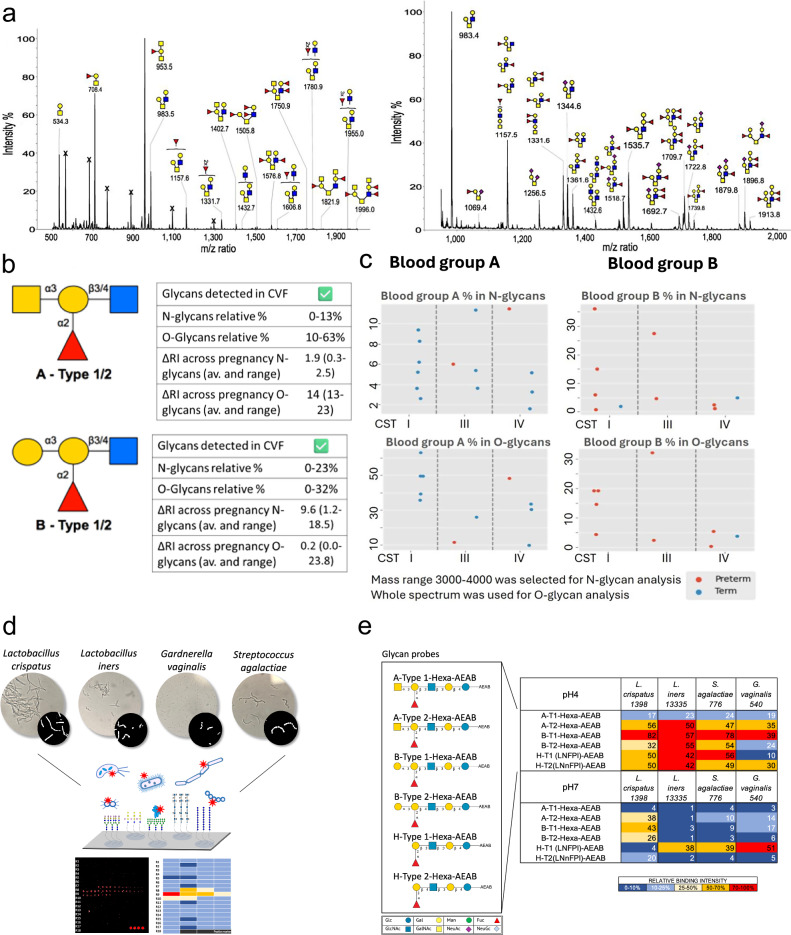
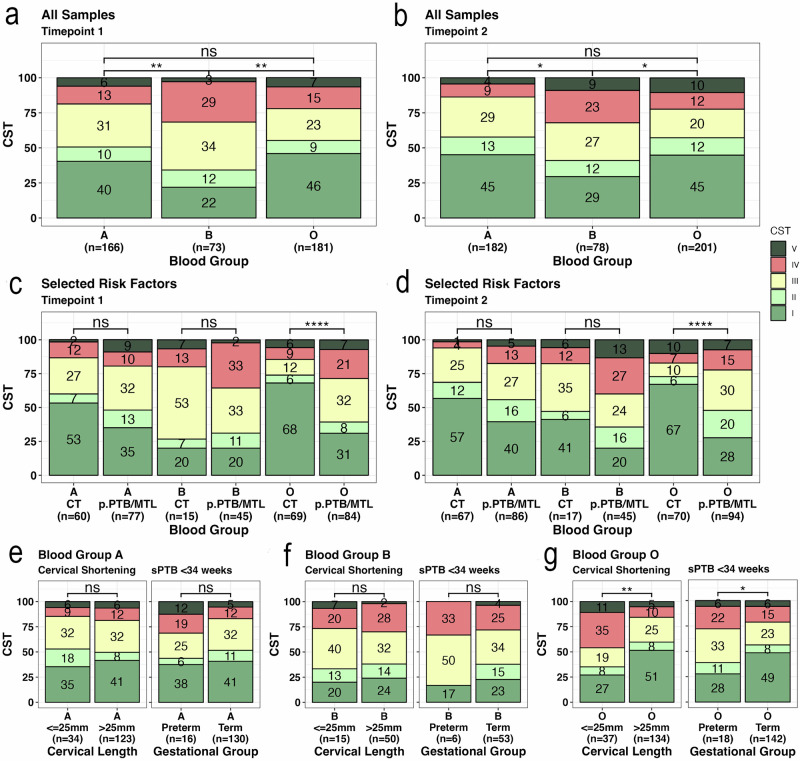
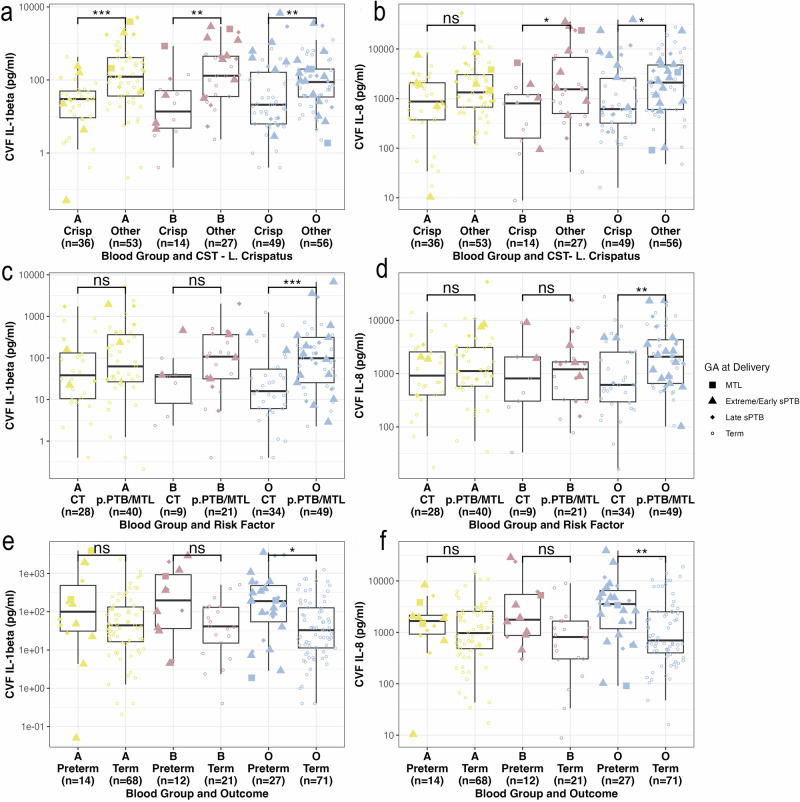
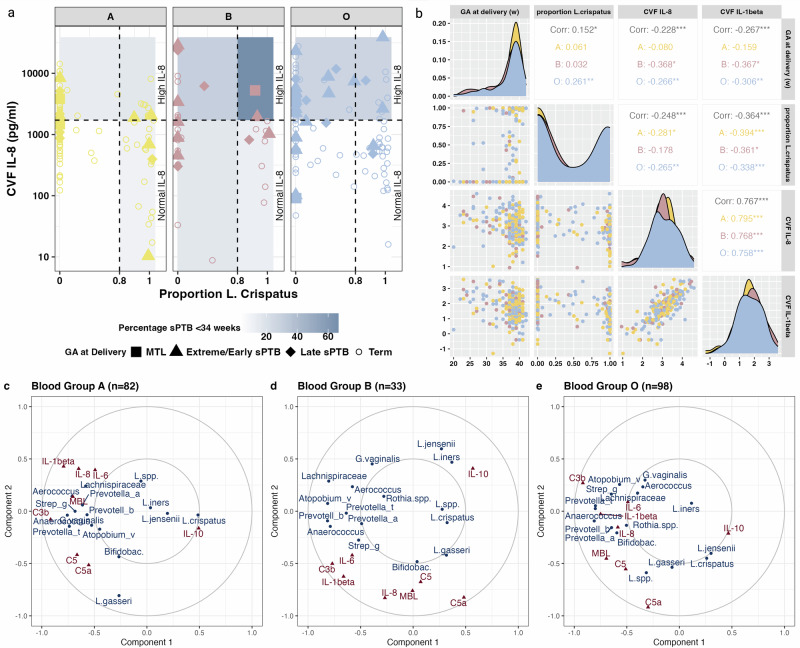
The mechanisms by which vaginal microbiota shape spontaneous preterm birth (sPTB) risk remain poorly defined. Using electronic clinical records data from 74,913 maternities in conjunction with metaxanomic (n = 596) and immune profiling (n = 314) data, we show that the B blood group phenotype associates with increased risk of sPTB and adverse vaginal microbiota composition. The O blood group associates with sPTB in women who have a combination of a previous history of sPTB, an adverse vaginal microbial composition and pro-inflammatory cervicovaginal milieu. In contrast, women of blood group A have a higher prevalence of vaginal Lactobacillus crispatus, a lower risk of sPTB, with sPTB cases showing no association with vaginal microbiota composition or inflammation. We found that cervicovaginal fluid contains ABH(O) glycans and shows variable binding to key vaginal bacteria. This indicates that cervicovaginal ABH(O) glycans influence microbiota-host interactions implicated in sPTB risk, suggesting a novel target for sPTB prediction and prevention.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures


References
-
- Ohuma, E. O. et al. National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. Lancet402, 1261–1271 (2023). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
