

Minimally invasive liver surgery for perihilar and intrahepatic cholangiocarcinoma: systematic review and meta-analysis of comparative studies
- PMID: 40931102
- PMCID: PMC12618328
- DOI: 10.1007/s00464-025-11900-4
Minimally invasive liver surgery for perihilar and intrahepatic cholangiocarcinoma: systematic review and meta-analysis of comparative studies
Abstract
Background: The implementation of minimally invasive liver surgery (MILS) for perihilar (PHC) and intrahepatic cholangiocarcinoma (IHC) remains limited and a systematic review including only comparative studies of MILS versus the open approach is lacking. This systematic review and meta-analysis aimed to assess the safety and efficacy of minimally invasive surgery in patients with hilar and intrahepatic cholangiocarcinomas.
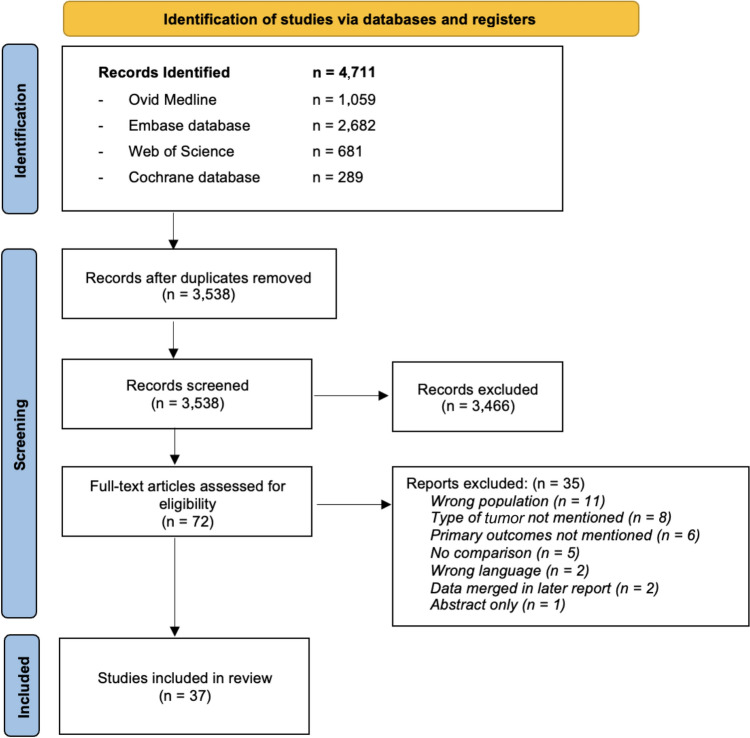
Methods: Systematic review in the PubMed, Embase, and Cochrane databases for original studies comparing at least five patients undergoing MILS with open liver surgery for PHC and IHC. Meta-analysis included the primary outcomes of morbidity and mortality. Secondary outcomes included post-operative outcomes, recurrence, disease-free survival, and resection margins.
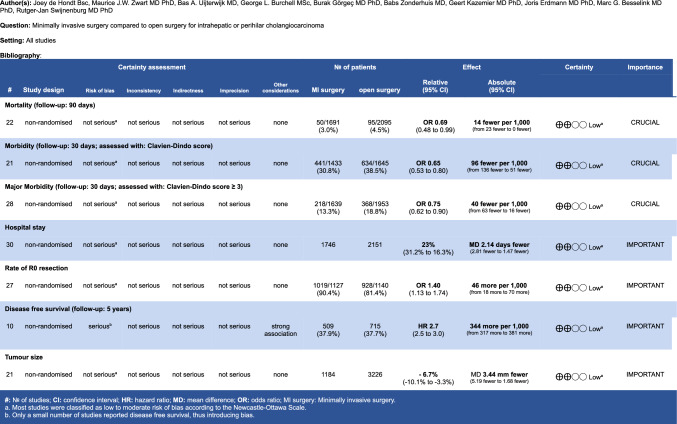
Results: Overall, 37 comparative non-randomised studies with 4863 patients were included, of which 24% PHC and 76% IHC. In 21 studies, propensity score matching was performed. In total, 2106 laparoscopic, 75 robotic, and 2662 open procedures were analysed. The conversion rate was median 11.5% [IQR 10.0-12.5]. MILS probably resulted in reduced rates of major morbidity, 13.3% vs 18.8% (OR 0.75, 95%CI 0.62-0.90), mortality, 3.0% vs 4.5% (OR 0.69, 95%CI 0.49-0.97), and shorter hospital stay, 8.0 vs 10.9 days (MD -2.1, 95%CI -2.8 - -1.5). MILS resulted in higher rate of R0 resections in PSM cohort, 90.4% vs 81.4%, (OR 1.40, 95%CI 1.13-1.74) and better 3-year disease-free survival rate (49.9% vs 38.5%, HR3-year 3.2, 95%CI 3.1-3.3). In the subgroup of 1180 patients in whom a hepatico-jejunostomy was performed (498 laparoscopic, 65 robotic, 617 open) MILS remained associated with reduced major morbidity, 20.9% vs 27.6% (OR 0.88, 95%CI 0.64-1.21) and resulted in better mortality, 4.2% vs 4.9% (OR 0.51, 95%CI 0.30-0.86), as compared to the open approach. Overall, the rate of biliary leakage was likely similar, 10.6% versus 11.7% (OR 0.83, 95%CI 0.52-0.77).
Conclusion: This systematic review of non-randomised comparative studies suggests that MILS for PHC and IHC may result in a similar safety profile with benefits in patient recovery and oncological outcomes as compared to OLS. Prospective comparative studies, especially including robotic MILS, are warranted.
Keywords: Cholangiocarcinoma; Hepatectomy; Minimally invasive; Robotic.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Disclosures: No specific funding was acquired for this study. Maurice J.W. Zwart and Marc G. Besselink received funding from the Amsterdam UMC for studies on safe implementation of robotic and laparoscopic pancreatic surgery; funding from the Dutch Digestive Foundation (MLDS; Grant Number I16-05), for studies on the aforementioned topics and funding from Intuitive (Grant Reference꞉ Evidence-based implementation of robotic pancreatoduodenectomy using simulation training, LAELAPS-3) for the nationwide Dutch LAELAPS-3 training program for robotic pancreatoduodenectomy. The other authors have nothing to disclose. Joey de Hondt, Bas A. Uijterwijk, George L. Burchell;, Burak Görgeç, Babs Zonderhuis, Geert Kazemier, Joris Erdmann, and Rutger-Jan Swijnenburg have no conflicts of interest or financial ties to disclose.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
