

Organ crosstalk: brain-lung interaction
- PMID: 40933561
- PMCID: PMC12417159
- DOI: 10.3389/fmed.2025.1655813
Organ crosstalk: brain-lung interaction
Abstract
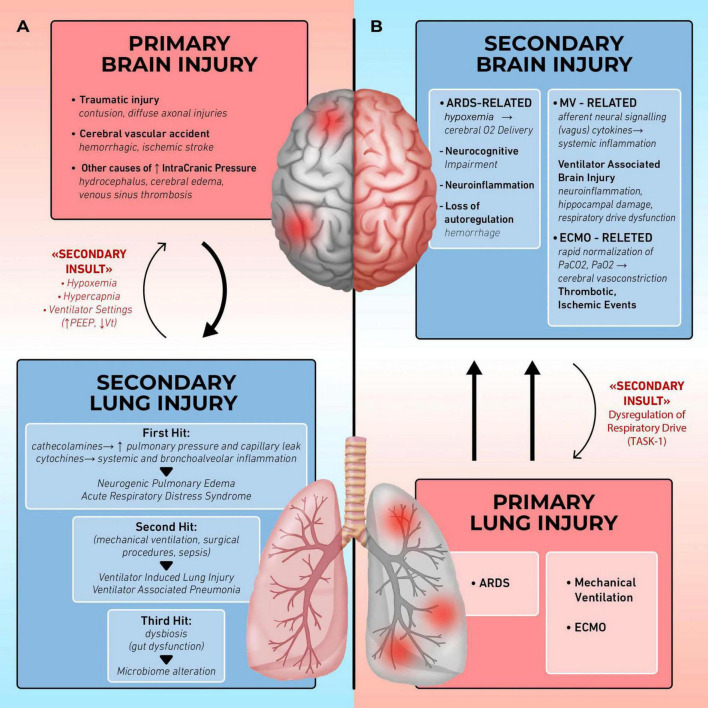
The interaction between the brain and the lungs is bidirectional: ICU patients with acute brain injury develop pulmonary complications, while ARDS patients frequently manifest neurological sequelae. Research is indeed focusing on both aspects of this cross-talk. On one side, ARDS survivors experience poor neurological outcomes both in the short and long term, with high incidence of delirium and post- discharge neurocognitive impairment. The underlying mechanisms have been investigated either in the pre-clinical and in the clinical field. Ventilator associated brain injury is the new recent term used to indicate the brain damage consequent to mechanical ventilation and leading to neuroinflammation and increased brain cells apoptosis. Moreover, prolonged hypoxia, deep sedation, loss of cerebral autoregulation and complications from vv-ECMO during ARDS are potentially sources of brain damage. On the other side, pulmonary complications in patients with acute brain injury follow a double-hit model, recently implemented in a triple-hit hypothesis. According to this theory, the primary brain injury leads to sympathetic hyperactivity, with inflammation and oxidative stress. Thus, the lungs become more vulnerable to develop complications such as neurogenic pulmonary edema and pneumonia. Finally, immune dysregulation and microbiome alterations due to brain-lung cross-talk lead to the worsening of lung injury. In this context, mechanical ventilation strategies aiming to guarantee adequate gas exchange and brain oxygen delivery are essential to prevent this phenomenon cascade. This review purpose is to examine the mechanisms behind brain-lung cross talk, starting from pathophysiological mechanisms, in order to suggest potential new research and therapeutic approaches.
Keywords: ARDS; acute brain injury; brain-lung cross talk; mechanical ventilation; neurogenic pulmonary edema; ventilator associated brain injury.
Copyright © 2025 Mascia, D’Albo, Cavalli, Giaccari, Della Giovampaola and Donati.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources