

Trends in maternal mortality and stillbirths by county in health facility data, Kenya, 2011-2022
- PMID: 40936076
- PMCID: PMC12427102
- DOI: 10.1186/s12884-025-07726-6
Trends in maternal mortality and stillbirths by county in health facility data, Kenya, 2011-2022
Abstract
Background: Reports on maternal deaths and stillbirths in health facilities are a critical but underutilized source of information to monitor the quality of care. In addition, with increasing coverage of deliveries by health facilities, such data can improve population estimates of maternal mortality and stillbirth rates. Data quality concerns, however, have often deterred use of facility data. This study aims to assess subnational trends in institutional mortality and examine its utility for improving population-based estimates of mortality.
Methods: Data from the routine monthly reporting system of the Ministry of Health in Kenya were used to assess levels and trends in maternal mortality and stillbirth rates in 47 counties from 2011 to 2022. Data quality was assessed using multiple methods, including consistency of annual reporting of live births, stillbirths and maternal deaths by counties, plausibility of the ratio of reported stillbirths to maternal death, the county institutional mortality in comparison to delivery coverage, socioeconomic development and health system characteristics. The consistency between institutional and population estimates of mortality was assessed using different scenarios.
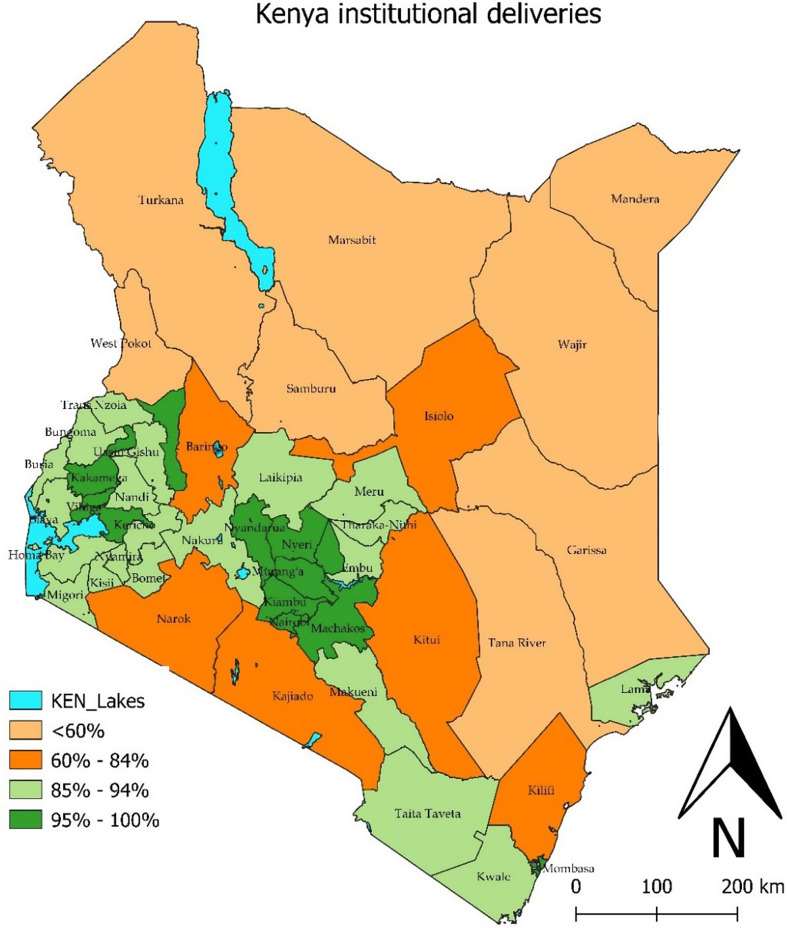
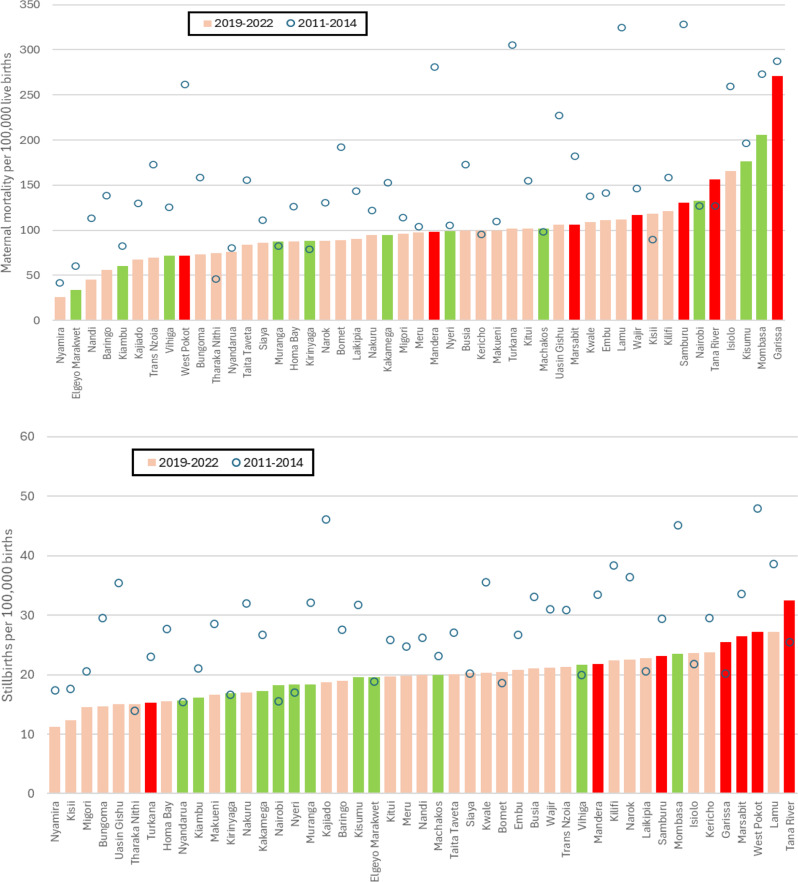
Results: Institutional live birth coverage increased from 64.0% in 2014 to 87.8% in 2022, ranging from 49 to 99% in counties. Kenya and 39 of its 47 counties experienced a decline in institutional maternal mortality ratio and stillbirth rate during the study period 2011-2022. The national institutional maternal mortality decline stagnated from 2018 and was 99 maternal deaths per 100,000 live births in 2022. Consistency of reported data by county was good over time but several indicators suggest that maternal death reporting was incomplete and more so in less-developed counties. Estimates of the population maternal mortality ratio, derived from the facility data, were much lower than global estimates or census results, while the stillbirth rates were consistent.
Conclusion: The health facility data on maternal death and stillbirths are an important data source for monitoring national and subnational institutional maternal mortality and stillbirth rates and can also inform population estimates. Systematic sustained assessment of reporting completeness will be critical to achieve the full potential of facility data-derived mortality monitoring.
Keywords: Data quality; Health facility data; Kenya; Maternal mortality; Stillbirths.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was based on secondary data analyses and no new data were collected. The Kenya Health Information System data used in the study are routinely collected as monthly aggregates from health facilities and counties by the Ministry of Health as part of its ongoing program management. No individual information is available in these data sets. Similarly, the program provided the data from the Maternal Death Surveillance and Response System at the aggregate level with no individual identifiers. Under the Ministry of Health practice, no ethical clearance is required for analyses of such data. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Ahmed S, Li Q, Scraford C, Pullum TW. An assessment of DHS maternal mortality data and estimates. DHS Methodological Reports No. 13. Rockville: ICF International; 2014.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
