

Biologic Footprint Reconstruction: Rotator Cuff Repair Using Biologic Tuberoplasty
- PMID: 40936580
- PMCID: PMC12420587
- DOI: 10.1016/j.eats.2025.103716
Biologic Footprint Reconstruction: Rotator Cuff Repair Using Biologic Tuberoplasty
Abstract
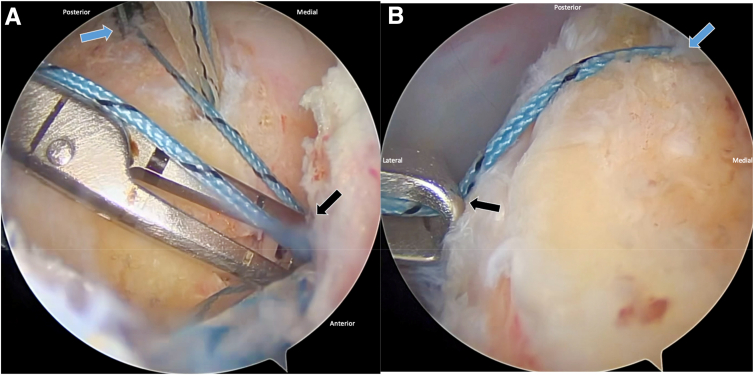
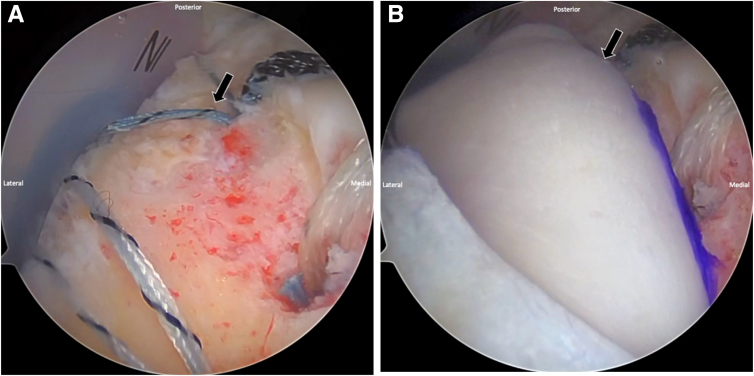
Irreparable rotator cuff tears present significant challenges owing to tear size, tendon retraction, and poor tissue quality. This article describes a surgical approach integrating biologic tuberoplasty with rotator cuff repair, using an acellular human dermal allograft to re-establish the rotator cuff footprint and prevent bone-on-bone contact between the humeral head and acromion. Footprint reconstruction is defined as allograft coverage of the tuberosity combined with partial cuff repair that includes some contact of the native cuff over the allograft. Changing the nomenclature to "biologic footprint reconstruction" more accurately describes the procedure when combined with partial cuff repair in continuity with the allograft and avoids confusion with isolated biologic tuberoplasty. The graft alleviates pain and creates a biologic healing environment. This approach is designed to reduce surgical complexity and improve efficiency, ensuring reproducibility while restoring shoulder biomechanics and function.
© 2025 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: K.A.B. reports a consulting or advisory relationship with Arthrex and Limacorporate; receives speaking and lecture fees from Arthrex; reports board membership with American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, and Ruth Jackson Orthopaedic Society; and owns equity or stocks in Limacorporate. R.M.F. reports board membership with American Academy of Orthopaedic Surgeons, American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, Arthroscopy Association of North America, International Cartilage Regeneration & Joint Preservation Society, International Society of Arthroscopy, Knee Surgery & Orthopaedic Sports Medicine, Journal of Shoulder and Elbow Surgery, and Orthopedics Today; reports a consulting or advisory relationship with AlloSource, Arthrex, and JRF Ortho; receives speaking and lecture fees from AlloSource, Arthrex, JRF Ortho, and Ossur; and receives funding grants from Arthrex. All other authors (E.H.R., D.J.S., P.A.S., D.R., P.B.M.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Yamamoto A., Takagishi K., Osawa T., et al. Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elbow Surg. 2010;19:116–120. - PubMed
-
- Tashjian R.Z. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin Sports Med. 2012;31:589–604. - PubMed
-
- Davies A., Singh P., Reilly P., Sabharwal S., Malhas A. Superior capsule reconstruction, partial cuff repair, graft interposition, arthroscopic debridement or balloon spacers for large and massive irreparable rotator cuff tears: A systematic review and meta-analysis. J Orthop Surg Res. 2022;17:552. - PMC - PubMed
LinkOut - more resources
Full Text Sources
