

Epilepsy and migraine: a diagnostic and therapeutic challenge
- PMID: 40949139
- PMCID: PMC12426056
- DOI: 10.3389/fphar.2025.1649543
Epilepsy and migraine: a diagnostic and therapeutic challenge
Abstract
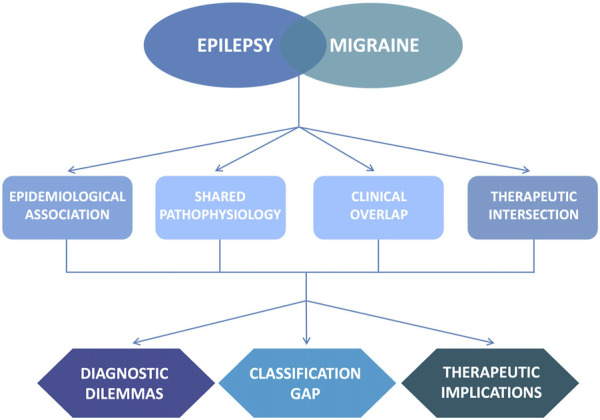
Migraine and epilepsy are two common, chronic, disabling, paroxysmal neurological disorders. A growing body of evidence from epidemiological, genetic, neurophysiological, and clinical research suggests a complex, bidirectional association between them. Migraine prevalence in epilepsy patients ranges from 8% to 23%, while the reverse is noted at 1%-17%. Both disorders are underpinned by cortical hyperexcitability, dysfunctional neurotransmission, and impaired ion homeostasis. Shared genetic mutations, particularly in genes encoding ion channel subunits such as CACNA1A, SCN1A, and ATP1A2, further support a common channelopathy model. Cortical spreading depression, the electrophysiological substrate of migraine aura, and paroxysmal depolarization shift, a hallmark of epileptic activity, share converging features, including neuronal depolarization, potassium accumulation, glutamate release, and eventual firing suppression. Glial dysfunction, glutamatergic excitotoxicity, and mitochondrial deficits are additional unifying elements. Clinically, the differential diagnosis between migraine with aura and focal seizures remains challenging due to overlapping sensory, visual, and autonomic symptoms. Rare phenomena including ictal epileptic headache, postictal headache, and migraine-triggered seizures further complicate the clinical spectrum. Additionally, certain epilepsy syndromes, such as childhood epilepsy, are strongly associated with migraine. Early recognition of comorbidity is crucial for appropriate management, as tailored treatment strategies may improve outcome. Several antiseizure medications, including topiramate, valproate, lamotrigine, and perampanel, also demonstrate efficacy in migraine prophylaxis. Moreover, non-pharmacological approaches such as ketogenic diet, vagus nerve stimulation, and transcranial magnetic stimulation provide further evidence of a shared neurobiological substrate. This review explores the epidemiological, pathophysiological, and clinical intersections between migraine and epilepsy, a frequent and clinically relevant dilemma. Accurate differentiation is urgently needed to avoid therapeutic delays or inappropriate interventions, given their phenotypic mimicry. In addition, it highlights therapeutic implications driven by overlapping molecular mechanisms. Ongoing research is needed to further elucidate this relationship.
Keywords: antiseizure medications; aura; headache; hemiplegic migraine; migralepsy; seizure.
Copyright © 2025 Pascarella, Marsico, Abelardo, Cutellè, Bulgari, Mummolo, Mammì, Cianci, Aguglia, Ferlazzo and Gasparini.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous