

Pediatric Meniscotibial Ligament Complex Anatomy and Biomechanics
- PMID: 40949534
- PMCID: PMC12426389
- DOI: 10.1177/23259671251367060
Pediatric Meniscotibial Ligament Complex Anatomy and Biomechanics
Abstract
Background: Meniscal repair is increasingly performed in pediatric patients, with capsular-based techniques remaining the gold standard despite limitations such as high failure rates and risk of meniscal extrusion. Recent studies highlight the potential role of accessory knee ligaments in improving meniscal stability and repair outcomes. The meniscotibial ligament complex (MTLC) has emerged as a potential area of interest to produce more normal anatomic and biomechanical meniscal function in meniscal repair.
Purpose: To evaluate the native anatomy and biomechanical strength of the MTLC of the medial and lateral meniscus of pediatric knees.
Study design: Descriptive laboratory study.
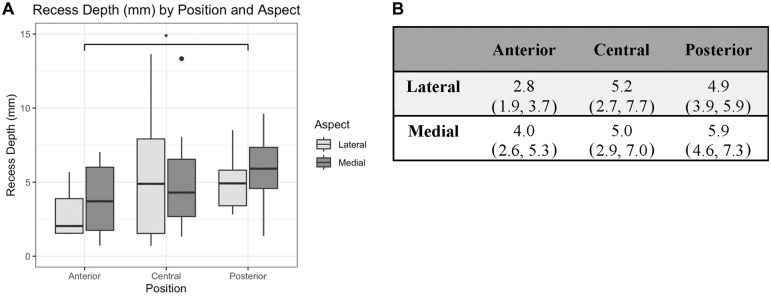
Methods: Fourteen fresh-frozen pediatric human knees (mean age, 7.5 years; range, 5-10 years; 6 male, 8 female) were used in this study. The depth of the recess between the MTLC and the meniscocapsular complex was measured. Subsequently, the medial and lateral menisci were divided into approximate thirds, creating anterior, central, and posterior testing zones for each meniscus. Each meniscus/MTLC complex underwent monotonic load-to-failure testing on an Instron 5944 test frame with a 2-kN load cell with load applied superiorly. Biomechanical properties were analyzed using linear mixed models with donor as a random factor and aspect (medial/lateral) and position (anterior/central/posterior) as fixed factors.
Results: The posterior recess depth was significantly larger (mean, 5.4 mm; 95% CI, 4.6-6.3 mm) than anterior (mean, 3.4 mm; 95% CI, 2.6-4.2 mm) (P = .049). Maximal load to failure in the posterior MTLC (mean, 93.5 N; 95% CI, 80.0-107.0 N) was significantly higher than anterior (mean, 69.2 N; 95% CI, 56.7-81.7 N) (P = .01).
Conclusion: This study defines a clear space in which the MTLC is distinct from the joint capsule, which is deepest in the posterior third of the medial and lateral meniscus. Our results demonstrate that the posterior region of the MTLC can withstand higher loads than the anterior region in pediatric knees.
Clinical relevance: These findings offer foundational insights into the native anatomy and biomechanics of the MTLC, guiding future studies involving the MTLC in meniscal repair. This knowledge may be particularly relevant to ramp lesions, other posterior meniscal tear patterns, and meniscal transplants.
Keywords: coronary ligament; meniscal instability; meniscal repair; meniscal tear; meniscotibial ligament complex; meniscus.
© The Author(s) 2025.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval was deemed not necessary for the present study.
Figures



References
-
- Abrams GD, Frank RM, Gupta AK, Harris JD, McCormick FM, Cole BJ. Trends in meniscus repair and meniscectomy in the United States, 2005-2011. Am J Sports Med. 2013;41(10):2333-2339. - PubMed
-
- Adams BG, Houston MN, Cameron KL. The epidemiology of meniscus injury. Sports Med Arthrosc Rev. 2021;29(3):e24. - PubMed
-
- Ahn JH, Bae TS, Kang KS, Kang SY, Lee SH. Longitudinal tear of the medial meniscus posterior horn in the anterior cruciate ligament–deficient knee significantly influences anterior stability. Am J Sports Med. 2011;39(10):2187-2193. - PubMed
-
- Bram JT, Mehta NN, Wright ML, Nguyen JC, Leska T, Ganley TJ. Pediatric ramp lesions. J Pediatr Orthop Soc N Am. 2020;2(1):48.
-
- Cavaignac E, Sylvie R, Teulières M, et al. What is the relationship between the distal semimembranosus tendon and the medial meniscus? A gross and microscopic analysis from the SANTI Study Group. Am J Sports Med. 2021;49(2):459-466. - PubMed
LinkOut - more resources
Full Text Sources
