

This is a preprint.
The potential impact, cost and cost-effectiveness of tuberculosis interventions - a modelling exercise
- PMID: 40950424
- PMCID: PMC12424940
- DOI: 10.1101/2025.09.02.25334943
The potential impact, cost and cost-effectiveness of tuberculosis interventions - a modelling exercise
Abstract
Background: While a range of interventions exist for tuberculosis prevention, screening, diagnosis, and treatment, their potential population impact and cost-effectiveness are seldom directly compared, or evaluated between settings with different background TB epidemiology and structural drivers.
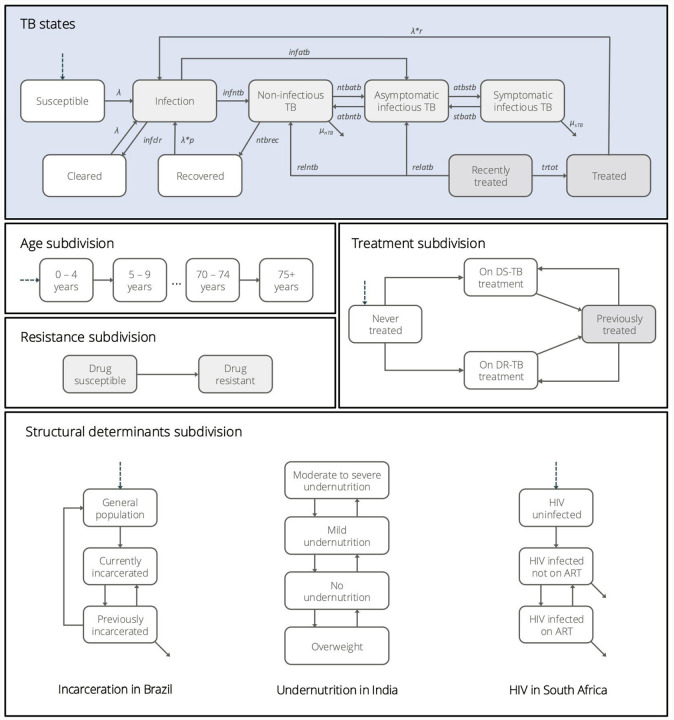
Methods: We calibrated a deterministic TB model to epidemiological indicators in Brazil, India, and South Africa. We implemented seven interventions across countries focusing on prevention, screening and diagnosis, and treatment of TB, as well as TB screening in prisons in Brazil and nutritional supplementation in India. We standardised scale-up (2025-2030), coverage (80% of target population), and strength of evidence for epidemiological impact using published efficacy data. We estimated epidemiological impact and incremental cost-effectiveness ratios (ICERs), expressed as costs per disability-adjusted life year (DALY) averted by 2050.
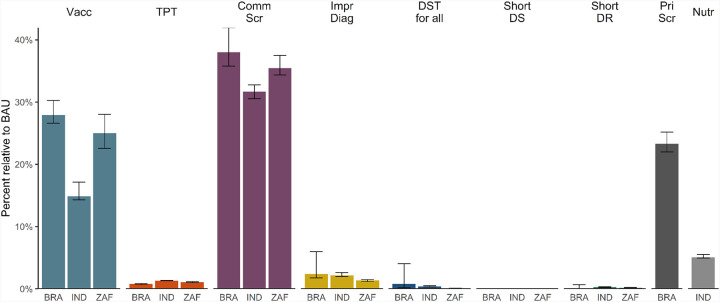
Results: Only three interventions prevented >10% of incident TB episodes by 2050: vaccination (median 15-28% across countries), symptom-agnostic community-wide screening (32-38%) and screening in prisons (23%). The impact of other interventions was more limited, ranging from 0% (shortened drug-susceptible treatment) to 5% (nutritional supplementation). ICERs varied widely by intervention and setting. Shortened drug-resistant treatment was cost-saving across settings, with the next lowest ICERs for prison screening in Brazil (72 USD/DALY) and nutritional supplementation in India (167 USD/DALY). Within each country, both low-cost community-wide screening and TB vaccine campaigns had lower USD/DALY than TB preventive treatment.
Conclusion: Interventions with meaningful epidemiological impact can also be cost-effective, but need to target populations beyond clinic-diagnosed individuals or their households. Achieving such potential requires a priority shift in funding, policy and product development.
Figures


References
-
- World Health Organisation. Global Tuberculosis Report. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/globa... (2024).
-
- Stover J. et al. The Effects of Reductions in United States Foreign Assistance on Global Health. SSRN Scholarly Paper at 10.2139/ssrn.5199076 (2025). - DOI
-
- Clark R. A. et al. The potential impact of reductions in international donor funding on tuberculosis in low-income and middle-income countries: a modelling study. Lancet Glob. Health 13, e1517–e1524 (2025). - PubMed
-
- Brink D. T. et al. Impact of an international HIV funding crisis on HIV infections and mortality in low-income and middle-income countries: a modelling study. Lancet HIV 12, e346–e354 (2025). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources