

Monocyte/macrophage-derived interleukin-15 mediates the pro-inflammatory phenotype of CD226+ B cells in type 1 diabetes
- PMID: 40957221
- PMCID: PMC12466144
- DOI: 10.1016/j.ebiom.2025.105946
Monocyte/macrophage-derived interleukin-15 mediates the pro-inflammatory phenotype of CD226+ B cells in type 1 diabetes
Abstract
Background: Type 1 diabetes (T1D) is characterised by the autoimmune-mediated destruction of pancreatic β-cells. Although traditionally viewed as a disease dominated by T cells, recent studies have emphasised the crucial role of B cells in the development of T1D. Genome-wide association studies (GWAS) have revealed that CD226 is related to susceptibility to several autoimmune diseases, including T1D. Our recent work identified a pathogenic role of CD226+ CD8+ T cells in T1D. However, the involvement of CD226+ B cells in T1D development remains unclear.
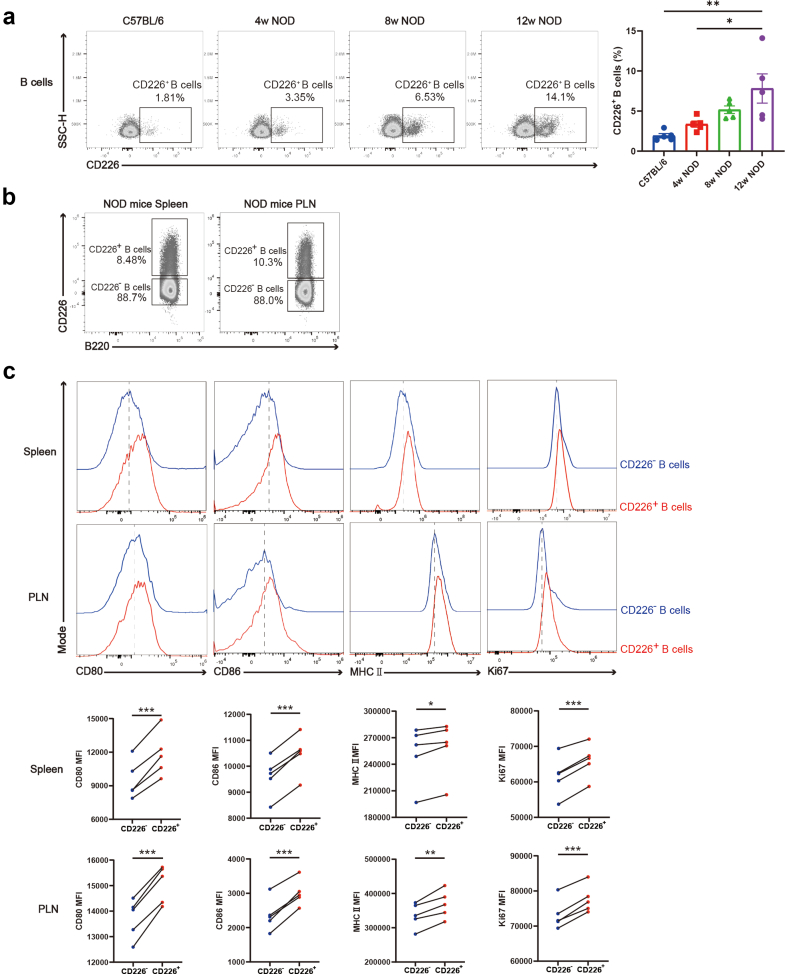
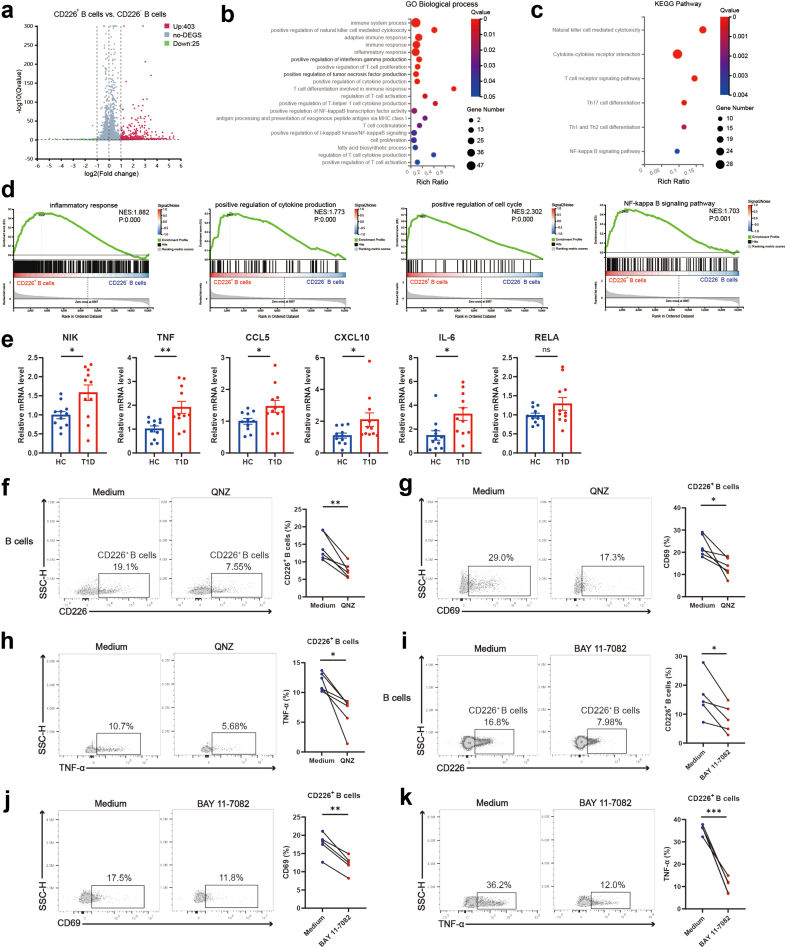
Methods: The expression and functional characteristics of CD226+ B cells in T1D patients and non-obese diabetic (NOD) mice were detected by flow cytometry. RNA sequencing and molecular biology experiments were performed to reveal regulatory mechanisms. In addition, in vivo interventions were conducted to explore potential preventive and therapeutic targets for T1D.
Findings: The percentage of CD226+ B cells is increased and positively correlated with disease severity in T1D. CD226+ B cells from T1D patients and NOD mice exhibit increased capability for activation, proliferation, and production of pro-inflammatory cytokines along with heightened glycolytic metabolism. Mechanistic studies have revealed that interleukin-15 (IL-15) secreted by monocytes or macrophages promotes the inflammatory response of CD226+ B cells. Importantly, the use of an anti-CD132 monoclonal antibody (anti-CD132) or an anti-IL-15 monoclonal antibody (anti-IL-15), which blocks IL-15 signalling, effectively prevented the disease onset of T1D. Furthermore, combination therapy with anti-CD3 monoclonal antibody (anti-CD3) and anti-CD132 synergistically reversed hyperglycemia in cyclophosphamide-accelerated NOD mice.
Interpretation: Our study demonstrates a novel role of the monocyte/macrophage-IL-15-CD226+ B cell axis in T1D immunopathogenesis and provides potential targets for T1D immunotherapy.
Funding: This work was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0507300, 2023ZD0507303, 2023ZD0508200, and 2023ZD0508201), the Natural Science Foundation of China (82570973, 82170795, 82470814, 82100949, and 82470931), the Scientific Research Program of FuRong Laboratory (2024PT5105) and the Central South University Research Programme of Advanced Interdisciplinary Studies (2023QYJC008).
Keywords: Autoimmune diabetes; B cells; CD226; Combination therapy; Type 1 diabetes.
Copyright © 2025 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declared that they have no conflict of interest.
Figures







References
-
- Quattrin T., Mastrandrea L.D., Walker L.S.K. Type 1 diabetes. Lancet. 2023;401(10394):2149–2162. - PubMed
-
- Roep B.O., Tree T.I. Immune modulation in humans: implications for type 1 diabetes mellitus. Nat Rev Endocrinol. 2014;10(4):229–242. - PubMed
-
- Lernmark A., Larsson H.E. Immune therapy in type 1 diabetes mellitus. Nat Rev Endocrinol. 2013;9(2):92–103. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
