

A pictorial essay of thoracic wall diseases: multiple pathologies in the same anatomical site
- PMID: 40975755
- PMCID: PMC12450195
- DOI: 10.1186/s13244-025-02073-8
A pictorial essay of thoracic wall diseases: multiple pathologies in the same anatomical site
Abstract
Objectives: To describe diagnostic and radiological features of the main pathologies affecting the thoracic wall, providing a pictorial atlas based on several clinical cases extracted from our archive.
Materials and methods: A wide variety of pathologies affect the tissues of the thoracic cage; these conditions are often encountered by radiologists during examinations performed for unrelated clinical questions. Modern imaging techniques enable the detection of these pathologies and allow definitive diagnoses to be achieved.
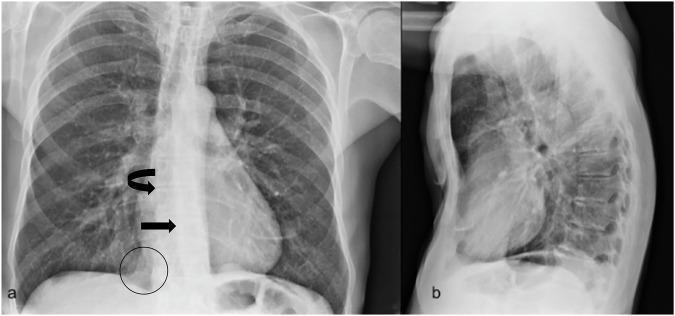
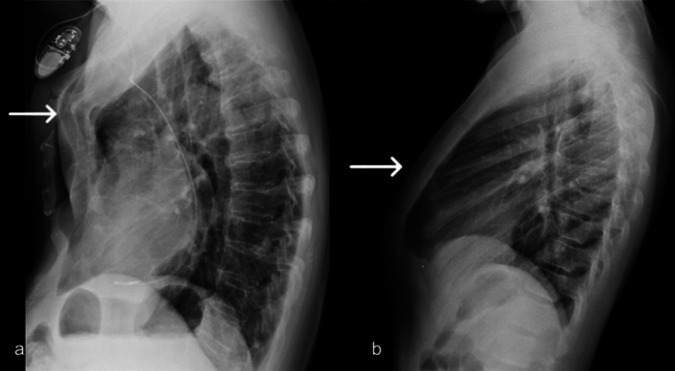
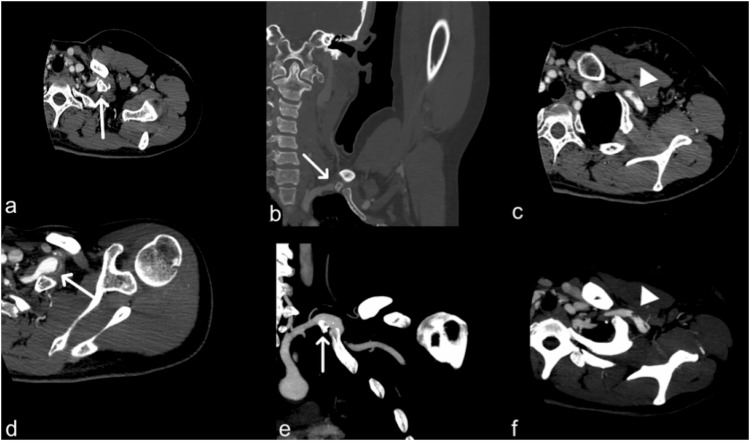
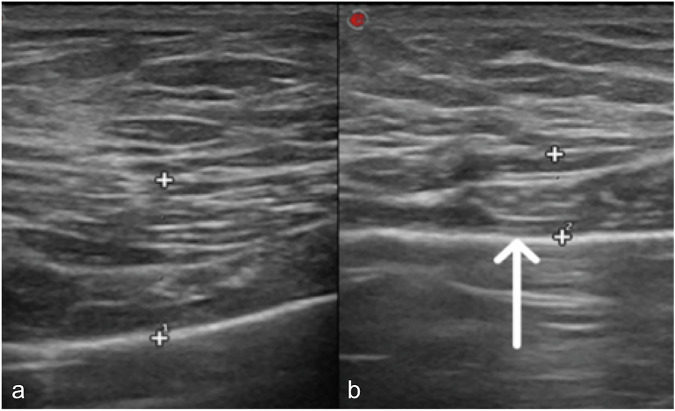
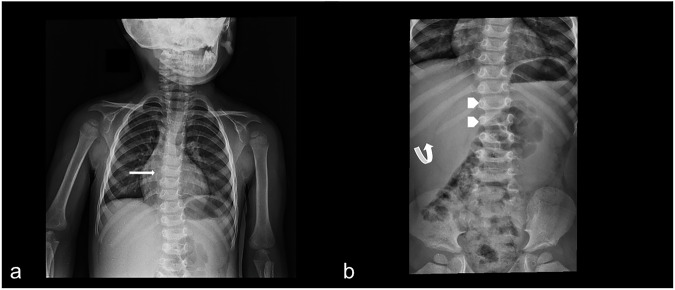
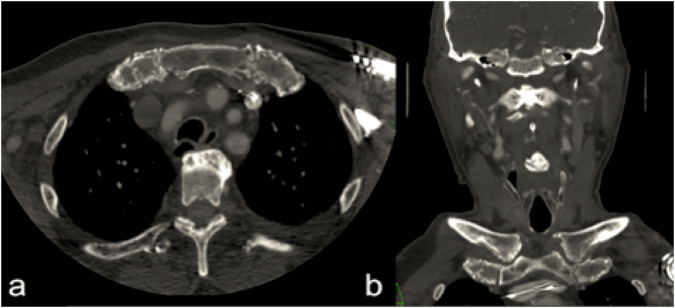
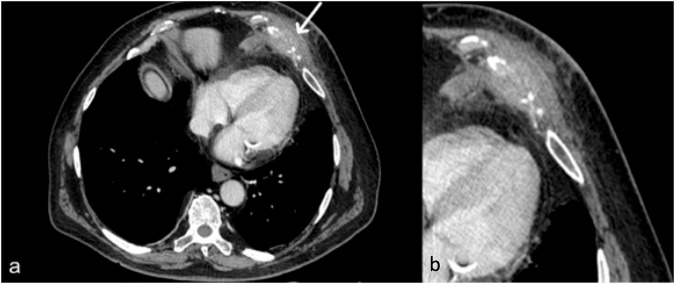
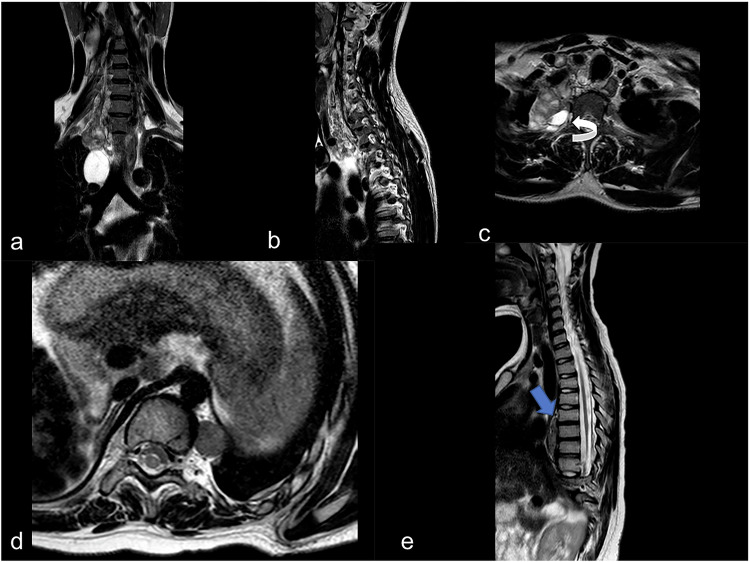
Results: Pathological processes that involve the chest wall may be classified into: (1) congenital and developmental diseases: pectus excavatum, pectus carinatum, supernumerary rib syndrome, Poland syndrome, neurofibromatosis, osteogenesis imperfecta, mucopolysaccharidosis, Marfan syndrome; (2) infectious and inflammatory diseases-such as aspergillosis, tuberculosis, abscesses from pyogenic bacteria, Tietze's syndrome; (3) bone injuries (traumatic and degenerative diseases): sternal, vertebral and costal fractures, degenerative disc and arthrosis pathology; (4) chest wall tumors-such as sarcomas, lymphomas, neurogenic tumors, lipoma.
Conclusions: Thoracic wall pathologies include a wide spectrum of conditions, with some clinical implications that often require a correct nosological framing. Recognizing these pathologies is essential for radiologists so that they can make a correct description in the report and direct toward appropriate treatment if required.
Critical relevance statement: Cage diseases are various and difficult to understand, so multimodality imaging plays a crucial role in achieving an efficient and final diagnosis.
Key points: Thoracic wall pathologies have different etiologies. Imaging represents a fundamental tool to clarify their extension, location, and nature. The prognosis of some of these diseases can be poor.
Keywords: Infections; Magnetic resonance imaging; Multidetector computed tomography; Neoplasms; Thoracic wall.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Anonymized use of these images for research and publication is covered by institutional policy. Competing interests: S.P. is a member of the scientific editorial board of Insights into Imaging (section: Abdominal) and, as such, did not participate in the selection or review processes for this article. The remaining authors declare that they have no competing interests related to this article.
Figures


References
-
- Dähnert W (2007) Radiology review manual 6th ed. Lippincott Williams & Wilkins, Philadelphia, PA
-
- Kelly RE, Cash TF, Shamberger RC et al (2008) Surgical repair of pectus excavatum markedly improves body image and perceived ability for physical activity: multicenter study. Pediatrics 122:1218–1222 - PubMed
-
- Garcia VF, Seyfer AE, Graeber GM (1989) Reconstruction of congenital chest-wall deformities. Surg Clin North Am 69:1103–1118 - PubMed
-
- Takahashi K, Sugimoto H, Ohsawa T (1992) Obliteration of the descending aortic interface in pectus excavatum: correlation with clockwise rotation of the heart. Radiology 182:825–828 - PubMed
-
- Haller JA, Kramer SS, Lietman SA (1987) Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg 22:904–906 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
