

Spatiotemporal multi-omics analysis uncovers NAD-dependent immunosuppressive niche triggering early gastric cancer
- PMID: 40976783
- PMCID: PMC12451012
- DOI: 10.1038/s41392-025-02390-w
Spatiotemporal multi-omics analysis uncovers NAD-dependent immunosuppressive niche triggering early gastric cancer
Abstract
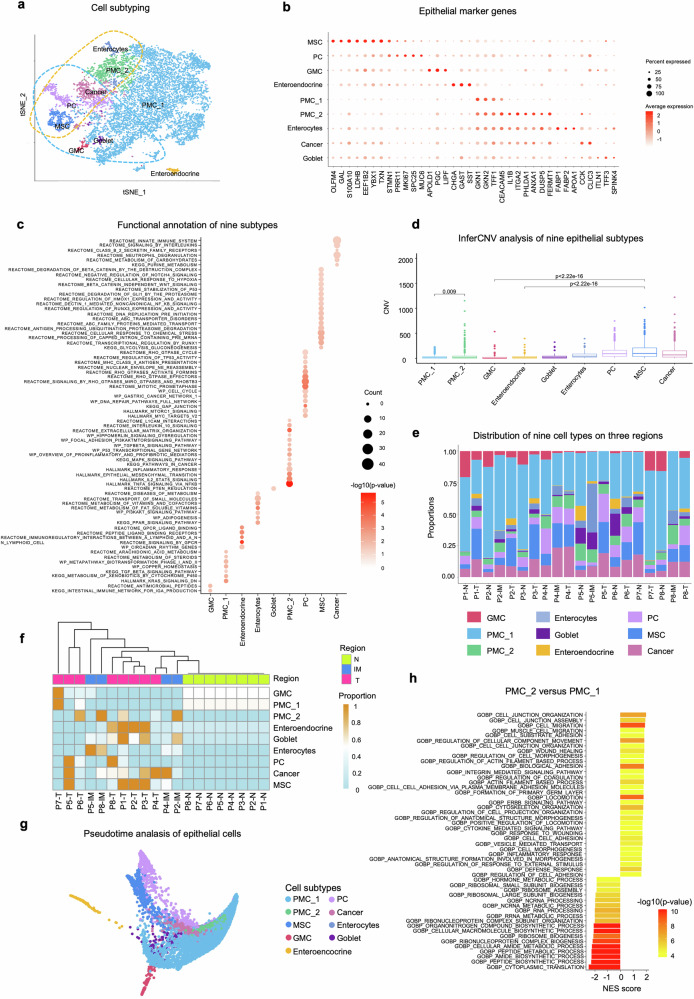
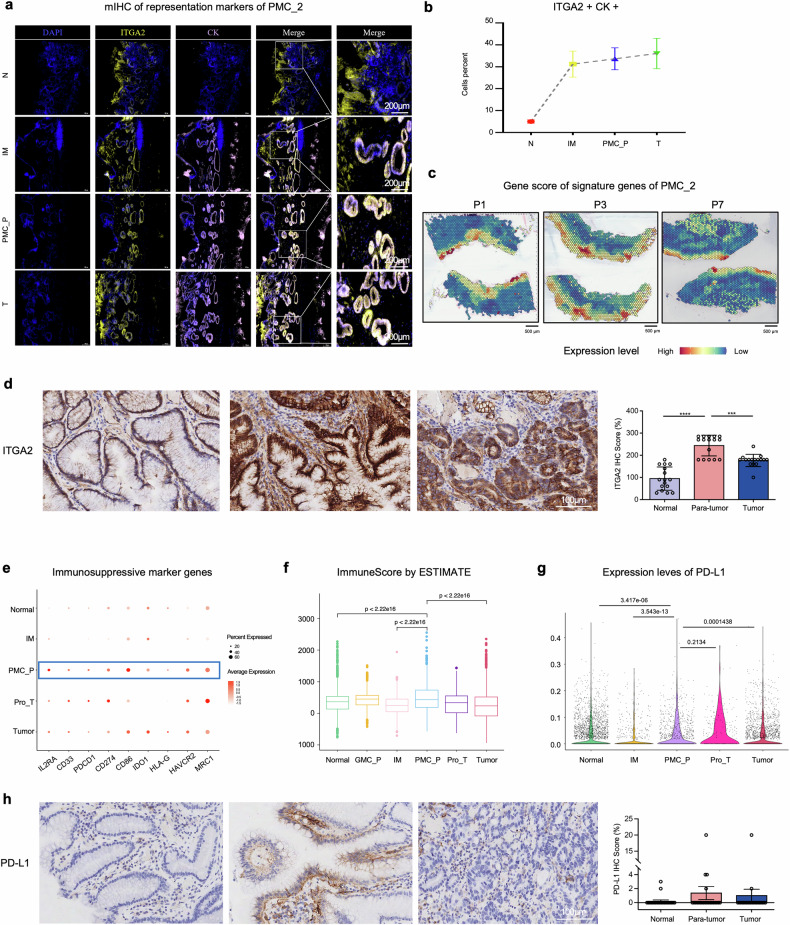
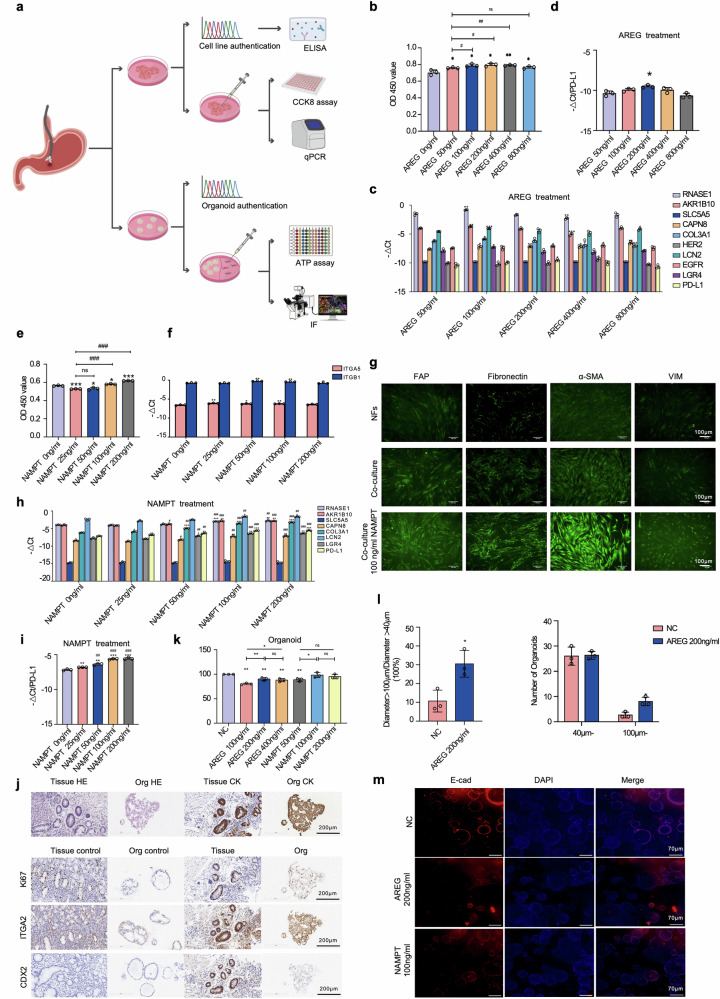
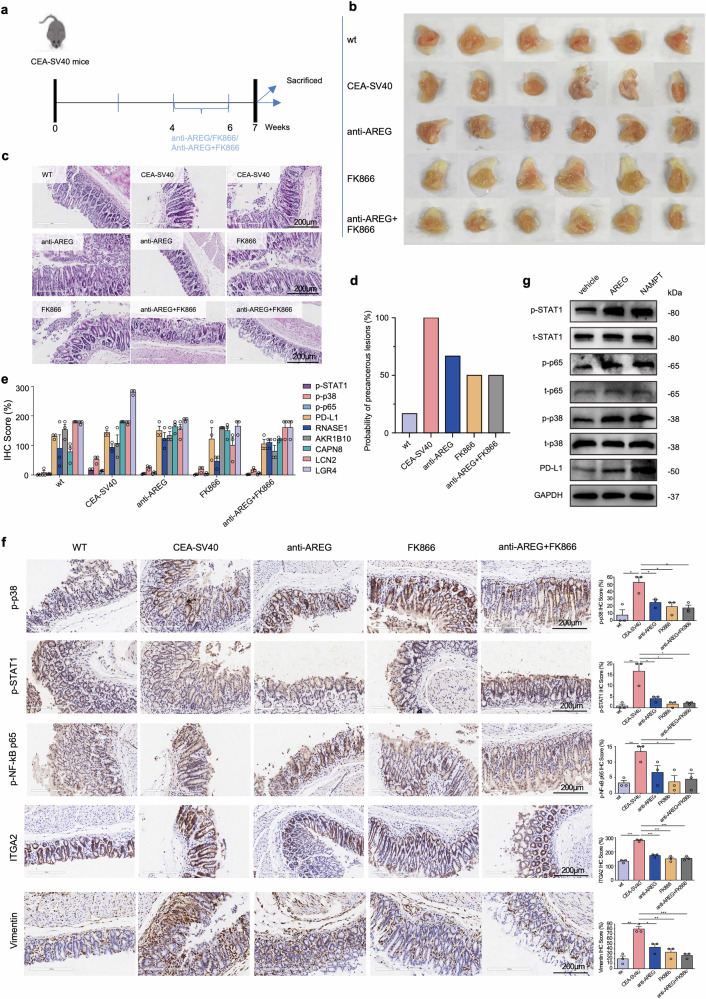
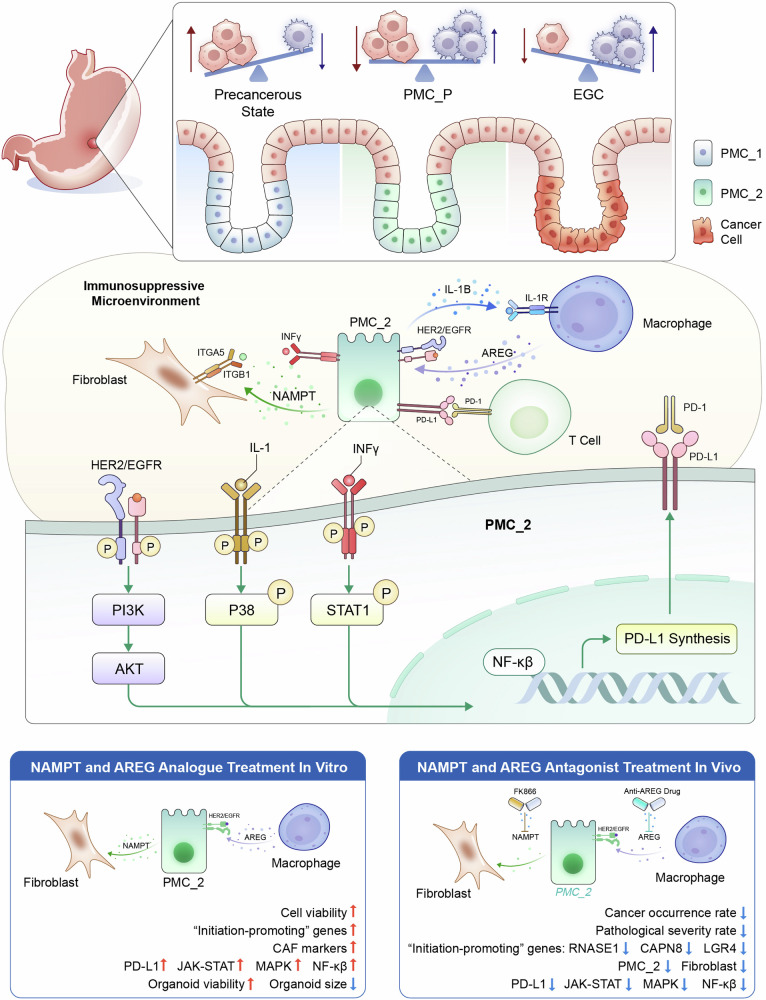
Understanding the cellular origins and early evolutionary dynamics that drive the initiation of carcinogenesis is critical to advancing early detection and prevention strategies. By characterizing key molecular, cellular and niche events at the precancerous tipping point of early gastric cancer (EGC), we aimed to develop more precise screening tools and design targeted interventions to prevent malignant transformation at this stage. We utilized our AI models to integrate spatial multimodal data from nine EGC endoscopic submucosal dissection (ESD) samples (covering sequential stages from normal to cancer), construct a spatial-temporal profile of disease progression, and identify a critical tipping point (PMC_P) characterized by an immune-suppressive microenvironment during early cancer development. At this stage, inflammatory pit mucous cells with stemness (PMC_2) interact with fibroblasts via NAMPT ITGA5/ITGB1 and with macrophages via AREG EGFR/ERBB2 signaling, fostering cancer initiation. We established gastric precancerous cell lines and organoids to demonstrate that NAMPT and AREG promote cellular proliferation in vitro. Furthermore, in the transgenic CEA-SV40 mouse model, targeting AREG and/or NAMPT disrupted key cell interactions, inhibited the JAK-STAT, MAPK, and NFκB pathways, and reduced PD-L1 expression, which was also confirmed by western blot in vitro. These interventions delayed disease progression, reversed the immunosuppressive microenvironment, and prevented malignant transformation. Clinical validation was conducted using endoscopically resected EGC specimens. Our study provides a precise spatiotemporal depiction of EGC development and identifies novel diagnostic markers and therapeutic targets for early intervention.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures




References
-
- Smyth, E. C. et al. Gastric cancer. Lancet396, 635–648 (2020).
-
- Correa, P. A human model of gastric carcinogenesis. Cancer Res.48, 3554–3560 (1988). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
