

The New WHO Cut-off Point for Defining High-altitude Anemia may be Inadequate
- PMID: 40977614
- PMCID: PMC12454947
- DOI: 10.1177/00469580251372827
The New WHO Cut-off Point for Defining High-altitude Anemia may be Inadequate
Abstract
Introduction: Peru carries a high burden of childhood anemia, particularly in high-altitude regions where hemoglobin (Hb) adjustment for altitude is recommended. This study aimed to evaluate whether the proportion of anemia attributable to iron deficiency (ID), inflammation, and red blood cell indices varies by altitude in children, using different diagnostic criteria.
Methods: We conducted a cross-sectional study of 280 children aged 6 to 72 months residing in Arequipa, Peru at altitudes ranging from 9 to 4310 m above sea level. Venous blood samples were collected to assess Hb, complete blood count, and serum biomarkers of iron status and inflammation. Spearman's rank correlation was used to examine relationships between altitude and hematologic or biochemical parameters. Logistic regression models evaluated associations between altitude, Hb concentration, and anemia prevalence, defined with and without altitude adjustment.
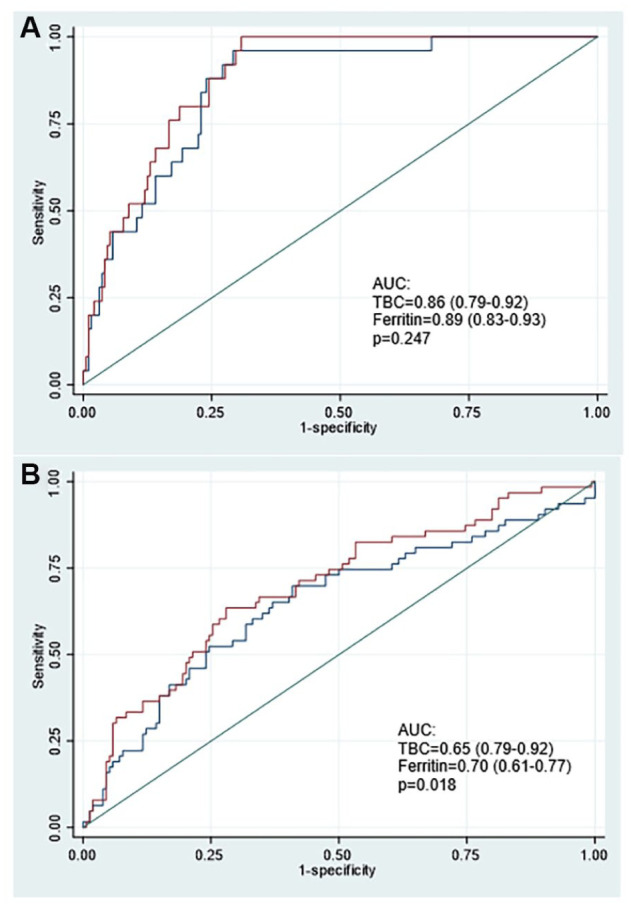
Results: Anemia prevalence increased from 12% to 31% after applying altitude-adjusted Hb thresholds. At mid-altitudes (1000-<3000 m), prevalence rose from 8.3% to 43.8% (P < .001), and at ≥3000 m, from 0% to 16.3% (P < .001). Overweight and obese children had a higher anemia prevalence using unadjusted Hb (28.6% vs 10.5%; P < .05), a difference that disappeared after adjustment. Iron deficiency was present in 5.6% of participants, while inflammation was detected up to 26.5%. Receiver operating characteristic (ROC) analysis indicated that unadjusted Hb thresholds had better diagnostic performance for identifying iron deficiency anemia (IDA) compared to altitude-adjusted definitions.
Conclusion: These findings suggest that altitude-adjusted Hb cutoffs may overestimate anemia prevalence and lead to misclassification of IDA in high-altitude pediatric populations.
Keywords: altitude; anemia; etiology; iron deficiency.
Conflict of interest statement
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


References
-
- World Bank. Prevalence of anemia among children (% of children ages 6–59 months) – Peru, Chile, Colombia, Ecuador, Bolivia, Argentina. World Bank Data. Updated 2024. Accessed July 15, 2025. https://datos.bancomundial.org/indicador/SH.ANM.CHLD.ZS?locations=PE-CL-...
-
- National Institute of Statistics and Informatics (INEI). Peru: Demographic and Family Health Survey 2023 (ENDES 2023). Lima, Peru: National Institute of Statistics and Informatics; 2024. Accessed July 18, 2025. https://www.inei.gob.pe
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
