

Hemiclamshell Resection of a Ruptured Mediastinal Teratoma Exhibiting Pancreatic Differentiation
- PMID: 40979262
- PMCID: PMC12444644
- DOI: 10.1002/rcr2.70345
Hemiclamshell Resection of a Ruptured Mediastinal Teratoma Exhibiting Pancreatic Differentiation
Abstract
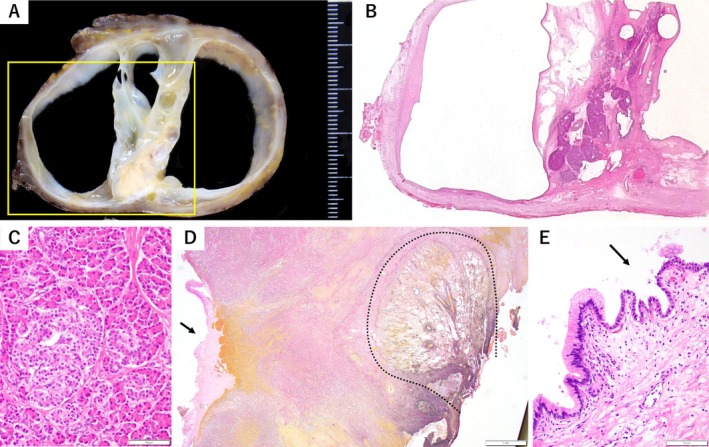
Mediastinal teratomas demonstrating unidirectional pancreatic differentiation are exceedingly rare. We describe a 36-year-old woman with progressively worsening anterior chest pain. Computed tomography demonstrated a 5.9 cm multilocular cystic mass in the anterior mediastinum, accompanied by pleural and pericardial effusions. Given the lesion's size and presumed inflammatory reaction, we performed radical excision via a hemiclamshell incision. Histopathology revealed predominantly pancreatic acinar tissue with scattered non-pancreatic epithelial elements, prompting reclassification as a mediastinal teratoma rather than ectopic pancreas. Focal epithelial disruption was regarded as the nidus of the surrounding inflammation. The patient's postoperative course was uneventful. This report underscores the need to include teratoma in the differential diagnosis of anterior mediastinal lesions initially interpreted as ectopic pancreas and illustrates the value of the hemiclamshell approach for achieving complete, atraumatic resection when extensive local adhesions are present.
Keywords: hemiclamshell approach; islets of Langerhans; mediastinal teratoma; pancreas; surgical resection.
© 2025 The Author(s). Respirology Case Reports published by John Wiley & Sons Australia, Ltd on behalf of The Asian Pacific Society of Respirology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- von Schweinitz D., Wittekind C., and Freihorst J., “Mediastinal Sequestration With Ectopic Pancreatic Tissue,” Zeitschrift für Kinderchirurgie 45, no. 4 (1990): 249–250. - PubMed
LinkOut - more resources
Full Text Sources
