

A Misleading Neck Mass: Branchial Cleft Cyst Mimicking Anaplastic Thyroid Carcinoma
- PMID: 40979824
- PMCID: PMC12449159
- DOI: 10.1210/jcemcr/luaf201
A Misleading Neck Mass: Branchial Cleft Cyst Mimicking Anaplastic Thyroid Carcinoma
Abstract
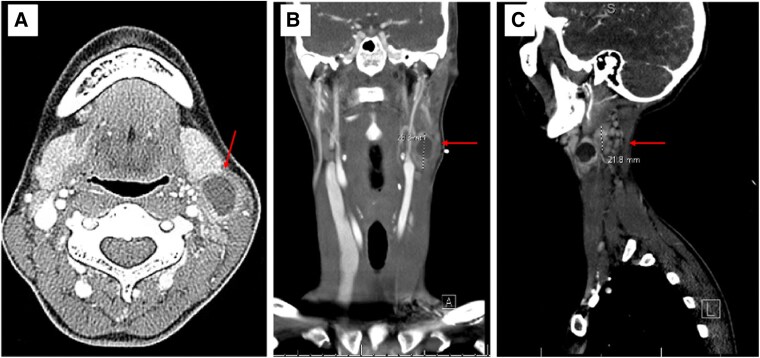
A 33-year-old female individual had a history of a lymph node excision positive for metastatic papillary thyroid carcinoma (PTC) in 2016. She was treated with a total thyroidectomy and central neck dissection showing 0.2-cm micro-PTC without paratracheal lymph node involvement, followed by adjuvant radioactive iodine treatment with 104 mCi of iodine-131. After 9 years without evidence of disease, she presented with a mildly tender, firm, left neck level II mass rapidly enlarging over 3 weeks. Neck ultrasound revealed a 3.5 cm irregular hypoechoic mass with internal vascularity and punctate echogenic foci. A fine needle biopsy showed inflammatory and mature squamous cells with elevated thyroglobulin but no definitive evidence of malignancy. The patient was scheduled for urgent neck dissection; however, just a left lymph node excision was performed as intraoperative frozen pathology showed no cancer. Surgical histopathology showed branchial cleft cyst tissue. The most concerning diagnosis for a rapidly enlarging neck mass in an adult with a history of metastatic PTC is anaplastic thyroid carcinoma. However, other diagnoses such as branchial cleft anomalies, lymphoma, or non-thyroid metastatic malignancies should be considered. Intraoperative frozen section pathology is crucial to direct surgical management of an unknown neck mass concerning for anaplastic thyroid cancer.
Keywords: anaplastic thyroid cancer; branchial cleft cyst; lymph node dissection; neck mass.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures


References
-
- Limaiem F, Kashyap S, Naing PT, Mathias PM, Giwa AO. Anaplastic Thyroid Cancer. StatPearls Publishing; 2025. Accessed July 11, 2025. http://www.ncbi.nlm.nih.gov/books/NBK538179/ - PubMed
-
- Rao SN, Smallridge RC. Anaplastic thyroid cancer: an update. Best Pract Res Clin Endocrinol Metab. 2023;37(1):101678. - PubMed
-
- Coste AH, Lofgren DH, Shermetaro C. Branchial Cleft Cyst. StatPearls. StatPearls Publishing; 2025. Accessed March 10, 2025. http://www.ncbi.nlm.nih.gov/books/NBK499914/ - PubMed
Publication types
LinkOut - more resources
Full Text Sources