

Polygenic scores contribution to Parkinson's disease comorbidities
- PMID: 40980402
- PMCID: PMC12448616
- DOI: 10.1093/braincomms/fcaf325
Polygenic scores contribution to Parkinson's disease comorbidities
Abstract
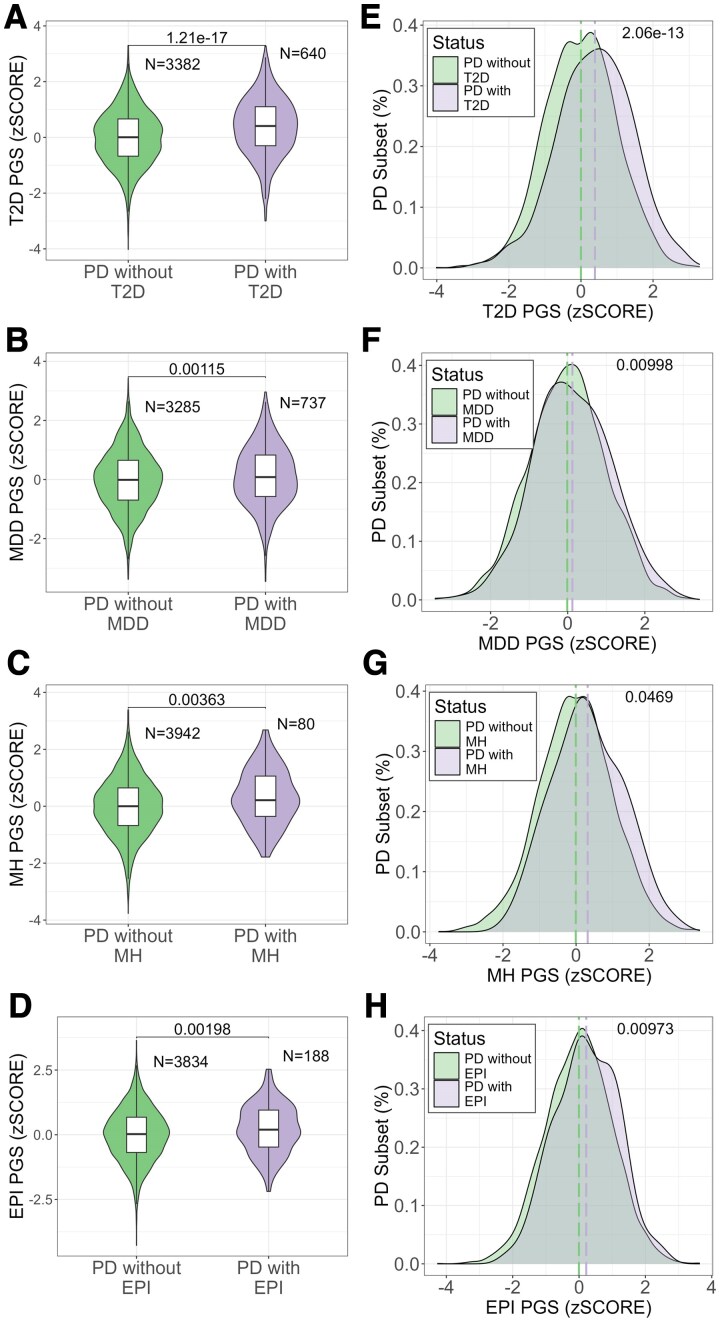
Comorbidities are common in Parkinson's disease and significantly impact the disease progression and management. While polygenic scores have been widely used to assess genetic risk for complex diseases, their role in comorbidity presentation in Parkinson's disease remains unclear. This study investigates whether genetic predisposition to comorbidities, as measured by polygenic scores, differs between individuals with Parkinson's disease and the general population and explores how genetic risk influences disease onset and sex-related differences. We analysed data from 4144 individuals with Parkinson's disease and 370 480 individuals from the general population in the UK Biobank, focusing on four comorbidities with high-quality genome-wide association study data: Type 2 diabetes, major depressive disorder, migraine headaches and epilepsy. We first compared polygenic score distributions between individuals with Parkinson's disease and the general population. While our findings indicate that comorbidities and polygenic risk scores do not significantly differ between individuals with Parkinson's disease and the general population, we show an association with disease onset and sex-specific differences. Individuals with earlier disease onset (50-70 years old) had higher genetic risk for major depressive disorder (odds ratio: 2.19, P-value: 1.27 × 10⁻¹⁵) and epilepsy (odds ratio: 1.58, P-value: 0.00845). Additionally, a female participant with Parkinson's disease exhibited higher genetic risk scores for major depressive disorder (odds ratio: 1.5, P-value: 0.0119) and migraine headaches (odds ratio: 2.1, P-value: 0.0155), while a male participant displayed higher genetic risk scores for Type 2 diabetes (odds ratio: 2.7, P-value: 2.11 × 10⁻¹⁷). Comorbidity-polygenic score did not differ between people with versus without Parkinson's disease, yet within Parkinson's disease, a higher genetic burden for specific comorbidities was linked to earlier onset and sex-specific presentation, implicating common variants as modifiers of clinical heterogeneity rather than the primary disease risk. These results enhance our understanding of the genetic influences shaping the broader clinical presentation of Parkinson's disease and highlight the need for further research into the interplay between genetic risk factors, comorbidities and disease heterogeneity.
Keywords: common variants; comorbidities; polygenic risk scores; polygenic scores.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report that they do not have competing interests.
Figures




References
-
- Pringsheim T, Jette N, Frolkis A, Steeves TDL. The prevalence of Parkinson’s disease: A systematic review and meta-analysis: PD PREVALENCE. Mov Disord. 2014;29(13):1583–1590. - PubMed
-
- Santos García D, Suárez Castro E, Expósito I, et al. Comorbid conditions associated with Parkinson’s disease: A longitudinal and comparative study with Alzheimer disease and control subjects. J Neurol Sci. 2017;373:210–215. - PubMed
-
- Leibson CL, Maraganore DM, Bower JH, Ransom JE, O’Brien PC, Rocca WA. Comorbid conditions associated with Parkinson’s disease: A population-based study: Comorbidity and Parkinson’s disease. Mov Disord. 2006;21(4):446–455. - PubMed
LinkOut - more resources
Full Text Sources