

Impact of vacuum assisted wound therapy on wound complications in STS surgery- A 3-year retrospective single-centre analysis
- PMID: 40996557
- PMCID: PMC12464026
- DOI: 10.1007/s00423-025-03865-8
Impact of vacuum assisted wound therapy on wound complications in STS surgery- A 3-year retrospective single-centre analysis
Abstract
Purpose: In sarcomas, surgery is an essential component of therapy. Depending on their location, sarcomas can reach a considerable size, which increases the risk of wound complications (WC) after resections. This often results in longer hospital stays and thus delays further oncological treatment. Therefore, reducing WCs is indispensable for improving treatment. The VAC (Vacuum-Assisted Closure) therapy has been shown to have a positive effect on wound healing, but there are limited studies for its use after sarcoma resections. The aim of this study was to analyze the outcomes of various wound closure techniques. This was intended to identify optimal wound care to prevent WCs and to determine risk factors for complications.
Methods: This study is a single-center study that included all patients who underwent surgery for sarcomas of the body surface and extremities. A retrospective data analysis was conducted for the years 2021-2023. The primary endpoint was the development of wound complications. Here, primary wound closure was compared with secondary closure after negative wound pressure therapy (NWPT). Secondary endpoints included the impact of drains, subtype, location, and comorbidities.
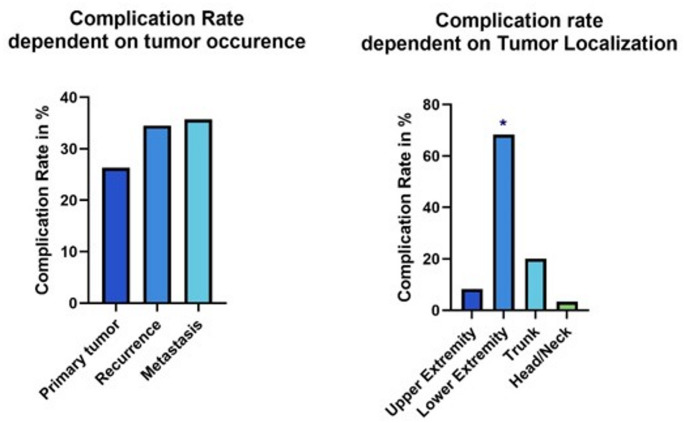
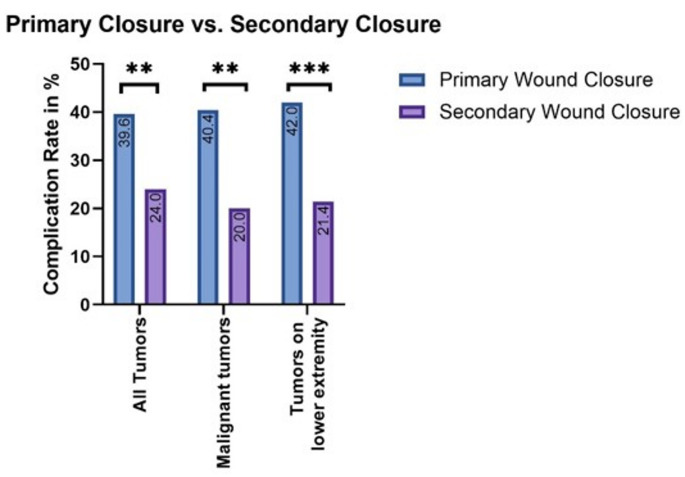
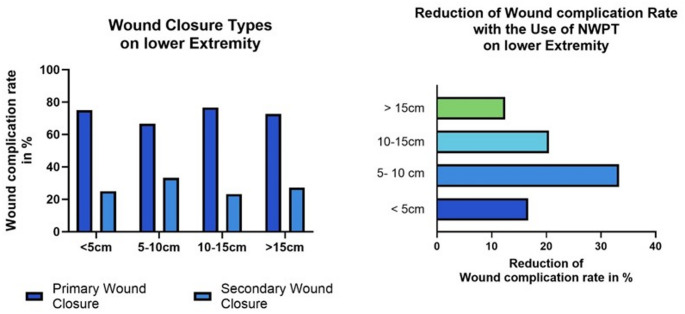
Results: A total of 211 patients were examined. The most common histological subtype was liposarcoma (32,88%), followed by undifferentiated sarcoma (19,18%). Wound complications occurred in 30,19% of all cases. The analysis showed that 40,4% of patients with primary wound closure developed a complication, while only 20% of patients with NWPT did. A significant risk factor for the development of a WC was a tumor diameter > 10 cm, which led to a 20,13% higher risk of infection compared to smaller tumors. 68.3% of wound complications occurred in the lower extremity. Additionally, neoadjuvant therapy, longer operation time and immunosuppression were detected as risk factors for a higher complication rate.
Conclusions: This study highlights the significantly increased risk of WCs in large sarcomas of the lower extremities. VAC therapy showed a significant improvement in wound closure especially in high-risk cases. Based on the results, the use of NWPT can be essential for wound management in sarcomas and improve convalescence and oncological treatment.
Keywords: Postoperative complications; Sarcoma surgery; Secondary wound closure; Soft tissue sarcoma; Vacuum assisted wound closure; Wound complication.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures



References
-
- Casali PG, Abecassis N, Bauer S et al (2018) Soft tissue and visceral sarcomas: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 29(May):iv51–iv67. 10.1093/annonc/mdy096 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
