

Obstructive sleep apnea mediates genetic risk of Diabetes Mellitus in Hispanic and Latino communities
- PMID: 40999017
- PMCID: PMC12462445
- DOI: 10.1038/s43856-025-01107-y
Obstructive sleep apnea mediates genetic risk of Diabetes Mellitus in Hispanic and Latino communities
Abstract
Background: Obstructive sleep apnea (OSA), and other sleep disorders, are associated with increased risk of developing diabetes mellitus (DM). We examined whether sleep disorders influence the genetic risk of developing diabetes in Hispanic/Latino individuals.
Methods: We developed Type 2 Diabetes (T2D) polygenic risk score (T2D-PRS) useful in admixed Hispanic/Latino individuals. We estimated the association of the T2D-PRS with cross-sectional (n = 12,342) and incident (n = 6965) DM in the Hispanic Community Health Study/Study of Latinos (ages 18-76, 50.9% female). We conducted a mediation analysis with T2D-PRS as an exposure, incident DM as an outcome, and OSA as a mediator. Additionally, we performed Mendelian randomization (MR) analysis to assess the causal relationship between T2D and OSA.
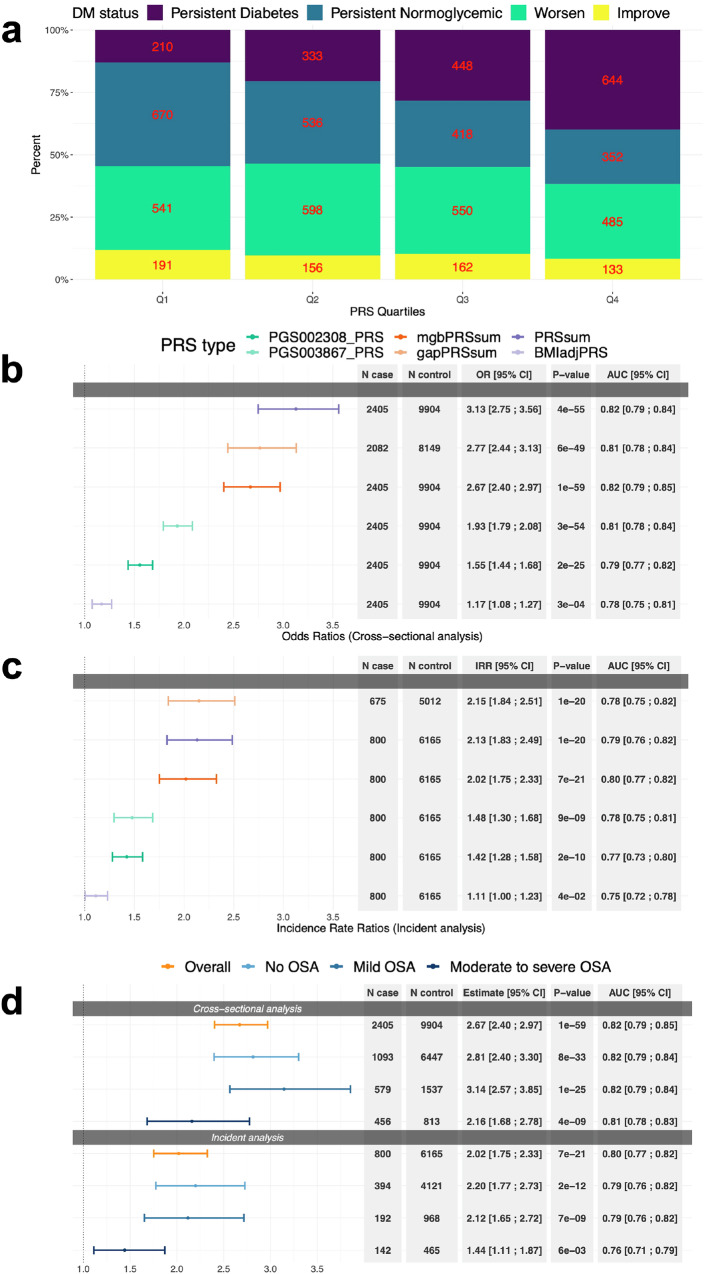
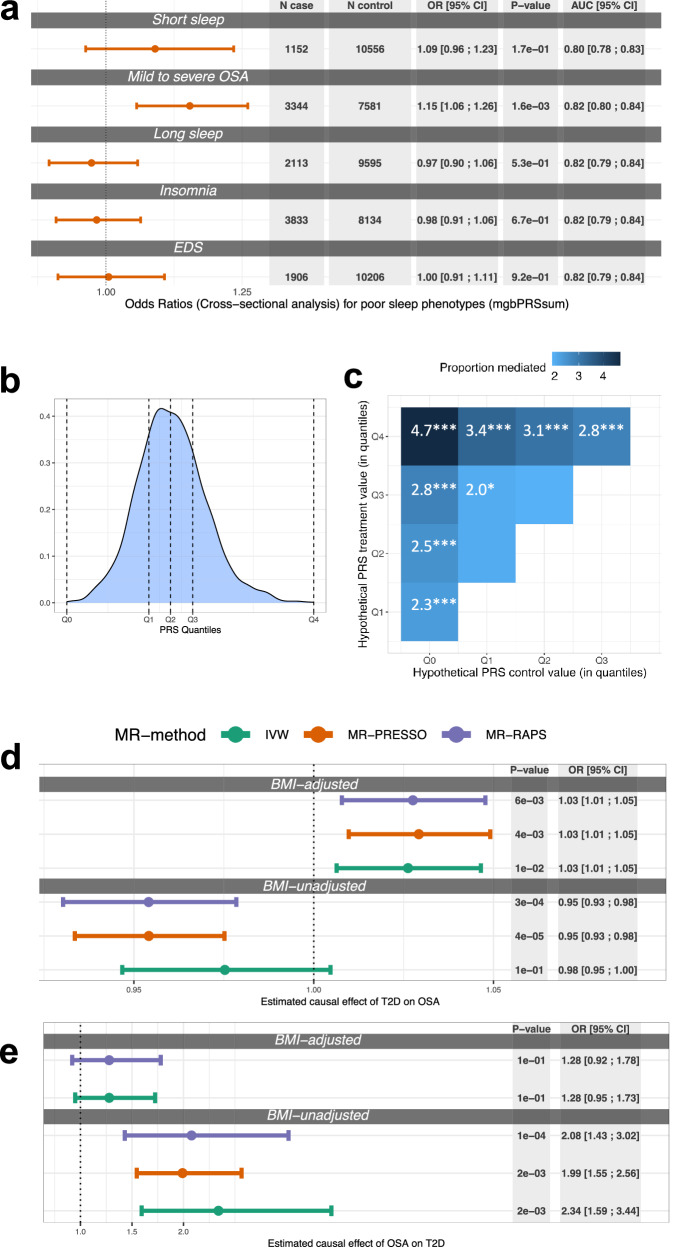
Results: Here, we show that a 1 standard deviation increase in T2D-PRS has DM adjusted odds ratio (OR) = 2.67, 95% CI [2.40; 2.97] and a higher incident DM rate (incident rate ratio (IRR) = 2.02, 95% CI [1.75; 2.33]). In a stratified analysis based on OSA severity categories the associations are stronger in individuals with mild OSA compared to those with moderate to severe OSA. Mediation analysis suggests that OSA mediates the T2D-PRS association with DM. In two-sample MR analysis, T2D has a causal effect on OSA, OR = 1.03, 95% CI [1.01; 1.05], and OSA has a causal effect on T2D, with OR = 2.34, 95% CI [1.59; 3.44].
Conclusions: These results support a causal association between OSA and DM, with OSA mediating up to 4.7% of the genetic risk for DM. OSA treatment may reduce DM prevalence.
Plain language summary
Sleep disorders such as obstructive sleep apnea play a role in diabetes. Here, we used genetic data to assess this role in over 12,000 Hispanic/Latino individuals. We developed a polygenic risk score summarizing genetic liability to diabetes, and showed that individuals with higher values of this genetic risk score are more likely to develop diabetes. We found that some of the genetic risk of diabetes is mediated via obstructive sleep apnea. Additionally, we implemented a genetic data analysis method called Mendelian randomization, finding that obstructive sleep apnea causally increases risk of diabetes. These results suggest that further studies should consider treating obstructive sleep apnea to potentially reduce diabetes prevalence.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Dr. Redline discloses consulting relationships with Eli Lilly Inc. Additionally, Dr. Redline serves as an unpaid member of the Apnimed Scientific Advisory Board, as an unpaid board member for the Alliance for Sleep Apnoea Partners and for the National Sleep Foundation. All other authors declare no competing interests.
Figures
Update of
-
Obstructive sleep apnea mediates genetic risk of Diabetes Mellitus: The Hispanic Community Health Study/Study of Latinos.medRxiv [Preprint]. 2024 Sep 10:2024.09.10.24313336. doi: 10.1101/2024.09.10.24313336. medRxiv. 2024. Update in: Commun Med (Lond). 2025 Sep 25;5(1):398. doi: 10.1038/s43856-025-01107-y. PMID: 39314966 Free PMC article. Updated. Preprint.
References
-
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care27, S5–S10 (2004). - PubMed
-
- Senaratna, C. V. et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med. Rev.34, 70–81 (2017). - PubMed
-
- Kono, M. et al. Obstructive sleep apnea syndrome is associated with some components of metabolic syndrome. Chest131, 1387–1392 (2007). - PubMed
Grants and funding
- HHSN268201300003I/HL/NHLBI NIH HHS/United States
- N01 HC065233/HL/NHLBI NIH HHS/United States
- N01 HC065236/HL/NHLBI NIH HHS/United States
- N01 HC065235/HL/NHLBI NIH HHS/United States
- R01 HL161012/HL/NHLBI NIH HHS/United States
- N01 HC065234/HL/NHLBI NIH HHS/United States
- R01HL161012/U.S. Department of Health & Human Services | NIH | National Heart, Lung, and Blood Institute (NHLBI)
- HHSN268201300003C/HG/NHGRI NIH HHS/United States
- N01 HC065237/HL/NHLBI NIH HHS/United States
- R35 HL135818/HL/NHLBI NIH HHS/United States
- R01 AG080598/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
