

Molecular genetic study of triploidy and the hydatidiform mole in pregnancy loss: analysis of 10,000 consecutive cases
- PMID: 41000402
- PMCID: PMC12457711
- DOI: 10.18699/vjgb-25-67
Molecular genetic study of triploidy and the hydatidiform mole in pregnancy loss: analysis of 10,000 consecutive cases
Abstract
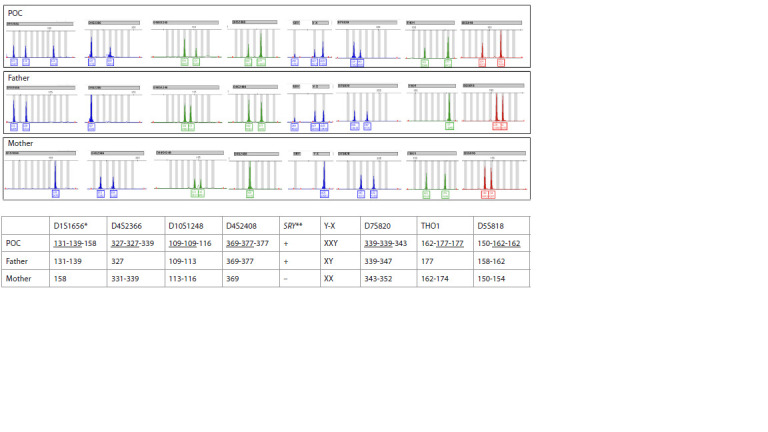
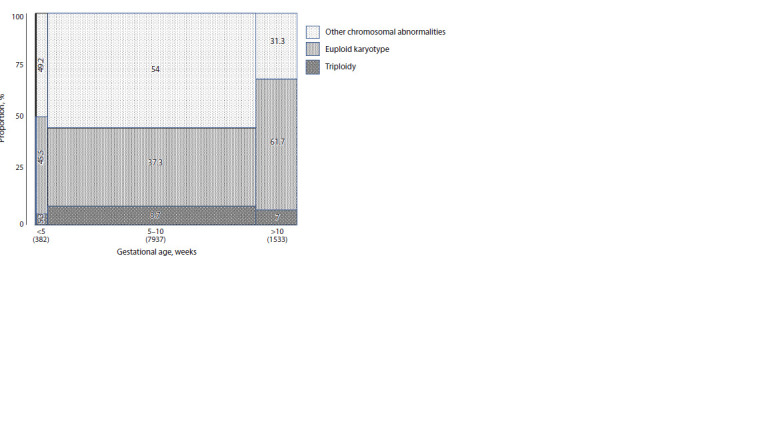
Approximately 10-15 % of clinically recognized pregnancies result in miscarriage, with chromosomal abnormalities identified in about 50 % of early pregnancy losses (PL). Triploidy accounts for approximately 12 % of all chromosomal abnormalities in miscarriages. The additional haploid set of chromosomes in triploidy may be of paternal (diandric triploidy) or maternal (digynic triploidy) origin. Diandric triploidy is associated with a partial hydatidiform mole (PHM), while pregnancies involving diploid embryos with two paternal genomes (and loss of the maternal nuclear genome) are the most common cause of a complete hydatidiform mole (CHM). The hydatidiform mole (HM) is the most prevalent form of gestational trophoblastic disease. Genotyping of products of conception (POC) is currently considered a reliable method for confirming HM and distinguishing its subtypes. The aim of this study was to use DNA genotyping of POCs to detect cases of triploidy, estimate the frequency of HM and its subtypes, and analyze the molecular and clinical characteristics of triploid pregnancies, CHM, and PHM in a Russian population. Between 2018 and 2024, a total of 10,000 consecutive PL cases were analyzed at the Medical Genetic Center Progen (Moscow). The main clinical indications included spontaneous miscarriage, missed miscarriage, and anembryonic pregnancy. DNA genotyping was performed using a five-color multiplex QF-PCR method, which included profiling of 26 autosomal STR markers, as well as DYS437, DXS6809, the SRY gene, and 30 markers from homologous regions located on different chromosomes. CHM was diagnosed based on the homozygosity of all STR markers. Triploidy was identified by analyzing peak area ratios of non-homozygous STR markers, which exhibited characteristic patterns of approximately 2:1 or 1:1:1. In our cohort, chromosomal abnormalities were identified in 58.8 % of all PL cases. Triploidy was detected in 8.3 % of the total sample, representing 14.3 % of all chromosomally abnormal POCs. Diandric triploidy accounted for 43 % of triploid cases. The prevalence of CHM was 0.11 %. The median age of women with triploidy was 32.1 years, and 27.9 years for those with CHM. Given the observed frequencies of PHM and CHM in our cohort, along with the relatively young maternal age associated with these conditions, enhancing current diagnostic protocols for HM - particularly through the incorporation of DNA genotyping of POCs - is essential for the effective prevention and timely diagnosis of post-molar malignant neoplasms in this population.
Из клинически признанных беременностей 10–15 % заканчиваются выкидышем, и около 50 % абортусов на ранних сроках беременности имеют хромосомные аномалии. Триплоидии составляют примерно 12 % от всех хромосомных аномалий абортусов. Дополнительный гаплоидный набор хромосом может быть отцовского (диандрическая триплоидия) или материнского происхождения (дигиническая триплоидия). Диандрическая триплоидия проявляется частичным пузырным заносом (ЧПЗ). Беременности диплоидными эмбрионами с двумя геномами отцовского происхождения (и потерей материнского ядерного генома) признаны наиболее частой причиной полного пузырного заноса (ППЗ). Пузырный занос (ПЗ) – это самый распространенный тип гестационной трофобластической болезни. Генотипирование абортусов в настоящее время рассматривается как надежный метод для подтверждения и дифференциальной диагностики подтипов ПЗ. Целью данного исследования было с помощью ДНК-генотипирования абортусов при невынашивании беременности (НБ) выявить случаи триплоидии, оценить частоту ПЗ, его подтипов, молекулярно- генетические и клинические особенности триплоидной беременности, ППЗ и ЧПЗ в российской популяции. С 2018 по 2024 г. в медико-генетическом центре «Проген» (Москва) были исследованы 10 000 последовательных случаев НБ. Основными направительными диагнозами являлись спонтанный выкидыш, неразвивающаяся беременность, анэмбриония. ДНК-генотипирование проводилось с помощью метода мультиплексной КФ- ПЦР, включавшего профилирование 26 аутосомных STR-маркеров, DYS437, DXS6809, SRY и 30 маркеров на гомологичных участках пар хромосом. Критерием ППЗ была гомозиготность всех STR-маркеров. Критерием триплоидии было соотношение площадей пиков всех негомозиготных STR-маркеров, близкое к 2:1 или 1:1:1. В нашей выборке из 10 000 случаев НБ аномальный кариотип абортусов был выявлен в 58.8 %, доля триплоидии составила 8.3 % от общего числа случаев или 14.3 % от абортусов с аномальным кариотипом. Доля диандрической триплоидии составила 43 %. Частота ППЗ была равна 0.11 %. Медианный возраст женщин с триплоидией был равен 32.1 года, с ППЗ – 27.9 года. Учитывая оцененную в нашей выборке частоту ЧПЗ и ППЗ и относительно молодой возраст женщин, у которых он встречался, необходимо совершенствовать имеющиеся методы диагностики ПЗ (включение ДНК-генотипирования) с целью адекватной профилактики и своевременной диагностики постпузырных злокачественных новообразований в данной возрастной группе.
Keywords: hydatidiform mole (complete and partial); miscarriage; quantitative fluorescent PCR (QF-PCR); short tandem repeats (STR); triploidy.
Copyright © AUTHORS.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




LinkOut - more resources
Full Text Sources