

The Right Approach: Power of Biomarkers in the Assessment and Management of Right Ventricular Dysfunction
- PMID: 41009628
- PMCID: PMC12469930
- DOI: 10.3390/ijms26189064
The Right Approach: Power of Biomarkers in the Assessment and Management of Right Ventricular Dysfunction
Abstract
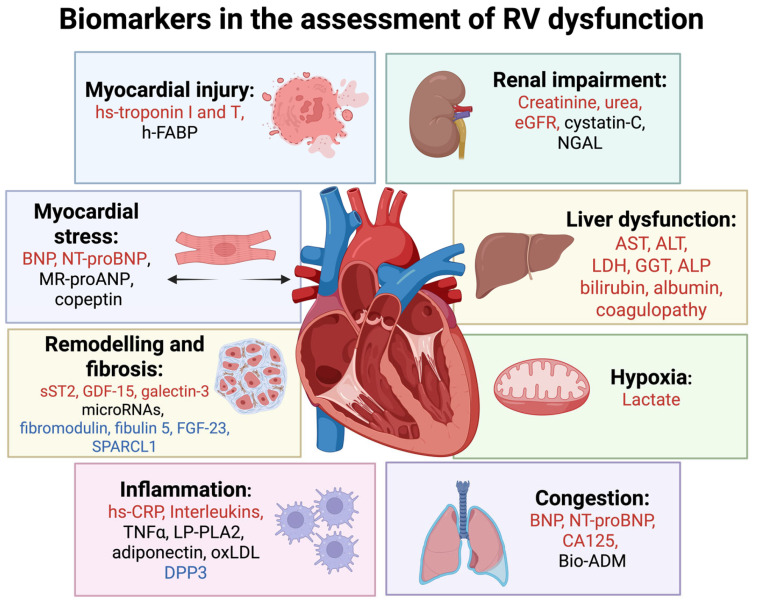
Right ventricular (RV) dysfunction is common and linked to poor outcomes across conditions such as heart failure (HF), acute coronary syndromes, pulmonary embolism, and pulmonary hypertension. While imaging, electrocardiogram (ECG), and invasive tests remain central to RV assessment, circulating biomarkers offer a rapid, non-invasive, and reliable alternative. These biomarkers reflect key pathophysiological processes, including myocardial injury, stress, fibrosis, inflammation, congestion, and multiorgan involvement. High-sensitivity troponins and natriuretic peptides (BNP, NT-proBNP) are already widely used, while emerging biomarkers-such as CA125, copeptin, galectin-3, and others-may enhance diagnostic accuracy and risk stratification. Some, like CA125 and NT-proBNP, have shown promise in guiding post-discharge therapy. However, challenges remain regarding the specificity of biomarkers for RV dysfunction and their role across different clinical contexts. This review provides an integrated overview of RV dysfunction, with a focus on the diagnostic and therapeutic potential of both established and novel biomarkers.
Keywords: acute myocardial infarction; biomarker; cardiovascular disease; diagnosis; dysfunction; heart failure; pulmonary embolism; pulmonary hypertension; right ventricle; risk stratification; therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Adamo M., Maccagni G., Fiorina C., Giannini C., Angelillis M., Costa G., Trani C., Burzotta F., Bruschi G., Merlanti B., et al. Prognostic value of right ventricle to pulmonary artery coupling in transcatheter aortic valve implantation recipients. J. Cardiovasc. Med. 2022;23:615–622. doi: 10.2459/JCM.0000000000001336. - DOI - PubMed
-
- Polovina M., Chioncel O., Savarese G., Abdelhamid M., Krljanac G., Tschöpe C., Seferović P. Predischarge and Postdischarge Heart Failure Management: Treatment Optimisation, Adherence, and Multidisciplinary Care. Med. Res. Arch. 2025;13 doi: 10.18103/mra.v13i5.6550. - DOI
-
- Harjola V.-P., Mebazaa A., Čelutkienė J., Bettex D., Bueno H., Chioncel O., Crespo-Leiro M.G., Falk V., Filippatos G., Gibbs S., et al. Contemporary management of acute right ventricular failure: A statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. Eur. J. Heart Fail. 2016;18:226–241. doi: 10.1002/ejhf.478. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
