

Risk Factors and Development of a Predictive Model for In-Hospital Mortality in Hemodynamically Stable Older Adults with Urinary Tract Infection
- PMID: 41011016
- PMCID: PMC12471474
- DOI: 10.3390/medicina61091625
Risk Factors and Development of a Predictive Model for In-Hospital Mortality in Hemodynamically Stable Older Adults with Urinary Tract Infection
Abstract
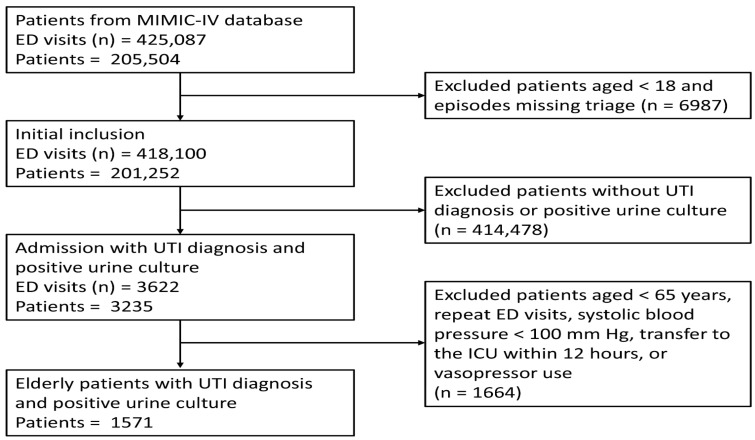
Background and Objectives: Urinary tract infections (UTIs) are a major cause of emergency department (ED) visits and hospital admissions among older adults. Although most seniors present hemodynamically stable, a sizeable fraction deteriorate during hospitalization, and no ED-specific tool exists to identify those at greatest risk. We sought to determine risk factors for in-hospital mortality in this population and to develop a predictive model. Materials and Methods: We analyzed the MIMIC-IV-ED database (2011-2019) and enrolled culture-confirmed UTI patients aged ≥ 65 years who were hemodynamically stable-defined as a systolic blood pressure ≥ 100 mm Hg without vasopressor support. Demographics, comorbidities, triage vital signs, and initial laboratory tests were extracted. Least Absolute Shrinkage and Selection Operator (LASSO) regression with 10-fold cross-validation was performed for variable selection. Discrimination was quantified with the C-statistic, calibration with the Hosmer-Lemeshow test, and clinical utility with decision curve analysis. Internal validation was assessed via 1000-sample bootstrap resampling. Results: Among 1571 eligible encounters (median age 79 years, 33% male), in-hospital mortality was 4.5%. LASSO selected eight variables; six remained significant in multivariable analysis: age, systolic blood pressure, oxygen saturation, white blood cell count, red cell distribution width, and blood urea nitrogen. The predictive nomogram demonstrated a C-statistic of 0.73 (95% CI 0.66-0.79) and outperformed traditional early warning scores. Conclusions: A six-variable nomogram may stratify mortality risk in hemodynamically stable older adults with UTI. Because the model was developed in a single U.S. tertiary-care ED, it remains hypothesis-generating until validated in external, multicenter cohorts to confirm generalizability.
Keywords: emergency department; older patient; predictive model; urinary tract infection.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
