

Serum chloride concentrations and outcomes in adult patients with cirrhosis: a systematic review and meta-analysis
- PMID: 41013381
- PMCID: PMC12465543
- DOI: 10.1186/s12882-025-04466-9
Serum chloride concentrations and outcomes in adult patients with cirrhosis: a systematic review and meta-analysis
Abstract
Purpose: Electrolyte disturbances, including hyponatremia, are common in cirrhosis, with hyponatremia already incorporated into the MELD-Na score as a prognostic marker. However, the prognostic role of serum chloride, the main extracellular anion, remains underexplored. Emerging evidence suggests hypochloremia is independently associated with increased mortality and acute kidney injury (AKI) in cirrhotic patients. Proposed mechanisms include dysregulated activation of the renin-angiotensin, vasopressin, and sympathetic nervous systems, leading to renal vasoconstriction and impaired function. This systematic review evaluates the association between serum chloride levels and outcomes, including mortality and KDIGO-defined AKI rates, aiming to enhance understanding and inform management strategies.
Methods: This review followed PRISMA guidelines and a PROSPERO-registered protocol (CRD42024550945). Comprehensive searches of MEDLINE, EMBASE, Cochrane, Scopus, and Web of Science were conducted through June 6, 2024, without language restrictions. Controlled vocabulary and keywords were used to identify relevant studies. Two independent reviewers performed title, abstract, and full-text screening, with disagreements resolved through consensus or third-party arbitration. Inter-rater reliability was assessed using Cohen's kappa. Data extraction and risk of bias evaluations were performed using the PROBAST tool. Findings were summarized using a PRISMA flowchart.
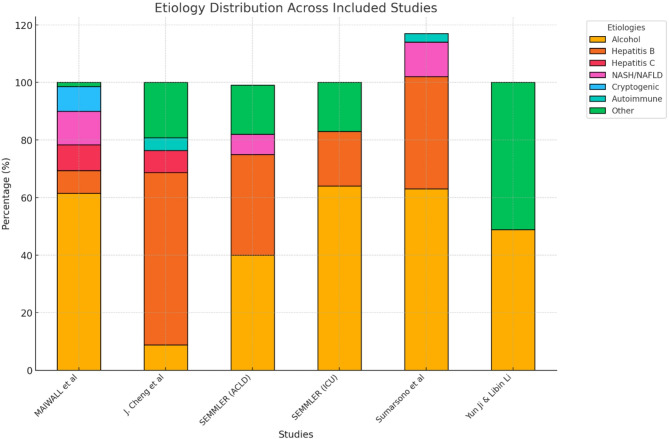
Results: Five studies (n = 3,150) were included, primarily retrospective cohorts, with one prospective study. Hypochloremia was defined as serum chloride < 99 mEq/L in most studies, except one, which used < 107.35 mmol/L. Cirrhosis etiologies included alcohol-related liver disease (40-64%), hepatitis B (7.9-59.9%), hepatitis C (7-8.9%), and non-alcoholic fatty liver disease (7-11.7%), with fewer cases of autoimmune and cryptogenic causes. Comorbidities included diabetes mellitus (21.3%), hypertension (13.4%), and varices (72-87%), with 62-99% having a history of decompensation. Extrahepatic organ failures were prevalent, affecting 79.4% of patients, with 31.6% and 13.4% experiencing two and three organ failures, respectively.Meta-analysis showed hypochloremia was significantly associated with increased mortality (pooled OR: 2.52; 95% CI: 1.88-3.39, p < 0.0001). Individual ORs ranged from 2.08 to 17.42, with low to moderate heterogeneity (I² = 36%). Hypochloremia also correlated with elevated creatinine levels and increased AKI prevalence.
Conclusion: Hypochloremia is a strong predictor of mortality and renal dysfunction in cirrhotic patients. Early recognition and management of hypochloremia are critical to improving outcomes in this high-risk population.
Clinical trial number: Not applicable.
Keywords: Acute kidney injury; Cirrhosis outcomes; Hypochloremia; Mortality risk; Serum chloride.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. This study involved analysis of previously published studies and did not require approval from an ethics committee. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Papper S. Fluid and electrolyte disturbances in cirrhosis. Am J Med Sci. 1976;272(1):53–6. - PubMed
-
- Lizaola B, Bonder A, Tapper EB, Mendez-Bocanegra A, Cardenas A. The changing role of sodium management in cirrhosis. Curr Treat Options Gastroenterol. 2016;14(2):274–84. - PubMed
-
- Gines P, Berl T, Bernardi M, Bichet DG, Hamon G, Jimenez W, et al. Hyponatremia in cirrhosis: from pathogenesis to treatment. Hepatology. 1998;28(3):851–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
