

Computational definition of medical exclusion and feasibility of excluding people not eligible for French population-based colorectal cancer screening from the French medico-administrative database
- PMID: 41013583
- PMCID: PMC12465781
- DOI: 10.1186/s12911-025-03175-5
Computational definition of medical exclusion and feasibility of excluding people not eligible for French population-based colorectal cancer screening from the French medico-administrative database
Abstract
Background: In the French population-based colorectal cancer screening program (CRCSP), the fact that the medical-exclusion rate was estimated only after a collection of voluntary statements from subjects could compromise an exhaustive collection of potential cases of medical-exclusion. The health insurance medico-administrative database (SNDS) that contains medical and healthcare consumption information have to date never been used to refine the target population of the CRCSP.
Objective: To identify in the SNDS, from published and disparate algorithms, the computational definitions of morbid situations that could justify medical exclusion from the CRCSP.
Methods: The non-systematic review of the literature synthetised an exhaustive list of algorithms targeting in SNDS, the morbid situations (CCR, colorectal adenoma/polyp, chronic inflammatory bowel disease, familial adenomatous polyposis, or Lynch syndrome colonoscopy, coloscanner, polypectomy) which may justify temporary or permanent medical exclusion from the CRCSP campaigns. Secondly, the discovered codes of morbid situations were searched on statistical reports to estimate their frequencies of use in SNDS (in 2021), and their interest in the computational phenotypes' algorithm.
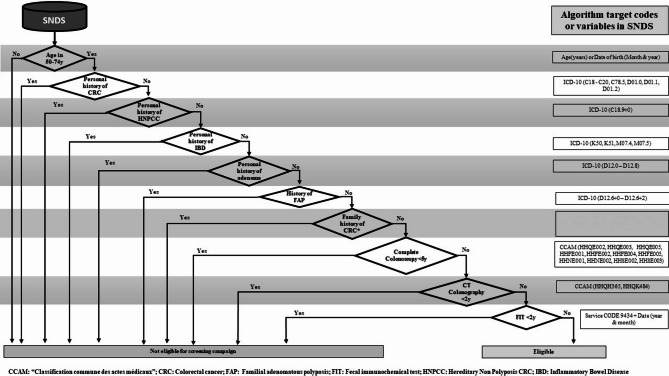
Results: The analysis of the literature (28 articles/studies) highlights the existence of diagnostic or therapeutic codes that can define in the SNDS database, the morbid situations justifying medical exclusion from the CRCSP. Except for personal or family history of CRC classifiable in the Z85.0 or Z80.0 codes of the ICD-10, almost all the morbid situations have a requestable definition in the SNDS. The target favoured by the search algorithms was the ICD-10 code (i.e., C18-C20, K50, K51). The definition codes listed were frequently used in SNDS in 2021, except for a few codes (D12.6 + 6, M07.5). From this definition of morbid situations by the only codes of the ICD-10 or the procedure codes emerges a feasibility and a decision-making algorithm for the choice of the person to be excluded from CRCSP campaign, using the SNDS. Age is the first discriminating variable in this decision-making algorithm because the CRCSP targeted people aged 50 to 74 years old and a restriction on age was made in several included SNDS's studies. The second discrimination based on diagnostic evidence derives its relevance from the quasi-systematic search for ICD-10 diagnostic codes in SNDS's studies.
Conclusion: In addition to being widely used in the context of medico-economic and epidemiological studies, the SNDS currently contains almost all the data essential for estimating the rate of medical-exclusion during colorectal cancer screening campaigns. While initiating the answer to the question of the choice of the most appropriate algorithm in each context, this review of the literature also emphasizes the need for validation studies because the quality of the algorithms used conditions the quality of the studies carried out in the medico-administrative databases.
Keywords: Colorectal cancer screening; Colorectal disease phenotype; Medical exclusion rate; Medico-administrative database; Participation rate.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Regulatory issues: All methods were carried out in accordance with relevant guidelines and regulations. According to the current French legislation, a study that does not change the care of patients does not require the opinion of the Clinical Research Center’s Ethics Committee. This article does not contain any studies with human participants performed by any of the authors. This study does not involve human participants, and informed consent was therefore not required. This article does not contain any studies with animals performed by any of the authors. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Hardcastle JD, Chamberlain JO, Robinson MH, Moss SM, Amar SS, Balfour TW et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996;348(9040):1472-7. 10.1016/S0140-6736(96)03386-7. PMID: 8942775. - PubMed
-
- JORF. Arrêté du 19 mars 2018 modifiant l’arrêté du 29 septembre 2006 relatif aux programmes de dépistage organisé des cancers et portant modification du cahier des charges du dépistage organisé du cancer colorectal. JORF n° 0068 du 22 mars 2018 texte n° 13. Journal Officiel de la République Française (JORF). 2018;0068:NOR: SSAP1807442A [Available from: https://www.legifrance.gouv.fr/loda/id/JORFTEXT000000460656/ ].
-
- Leuraud K, Jezewski-Serra D, Viguier J, Salines E. Colorectal cancer screening by guaiac faecal occult blood test in France: Evaluation of the programme two years after launching. Cancer Epidemiol. 2013;37(6):959 – 67. 10.1016/j.canep.2013.07.008. PMID: 24035240. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
