

Genetic Landscape of Opsoclonus-Myoclonus-Ataxia Syndrome in Children
- PMID: 41014805
- PMCID: PMC12476522
- DOI: 10.1016/j.pediatrneurol.2025.08.019
Genetic Landscape of Opsoclonus-Myoclonus-Ataxia Syndrome in Children
Abstract
Background: Opsoclonus-myoclonus-ataxia syndrome (OMAS) is a rare neurological disorder, with involuntary rapid saccadic conjugate eye movements as one of characteristics, primarily affecting the cerebellum. While the exact pathogenesis remains unclear, genetic and autoimmune factors have been suggested to contribute to its development.
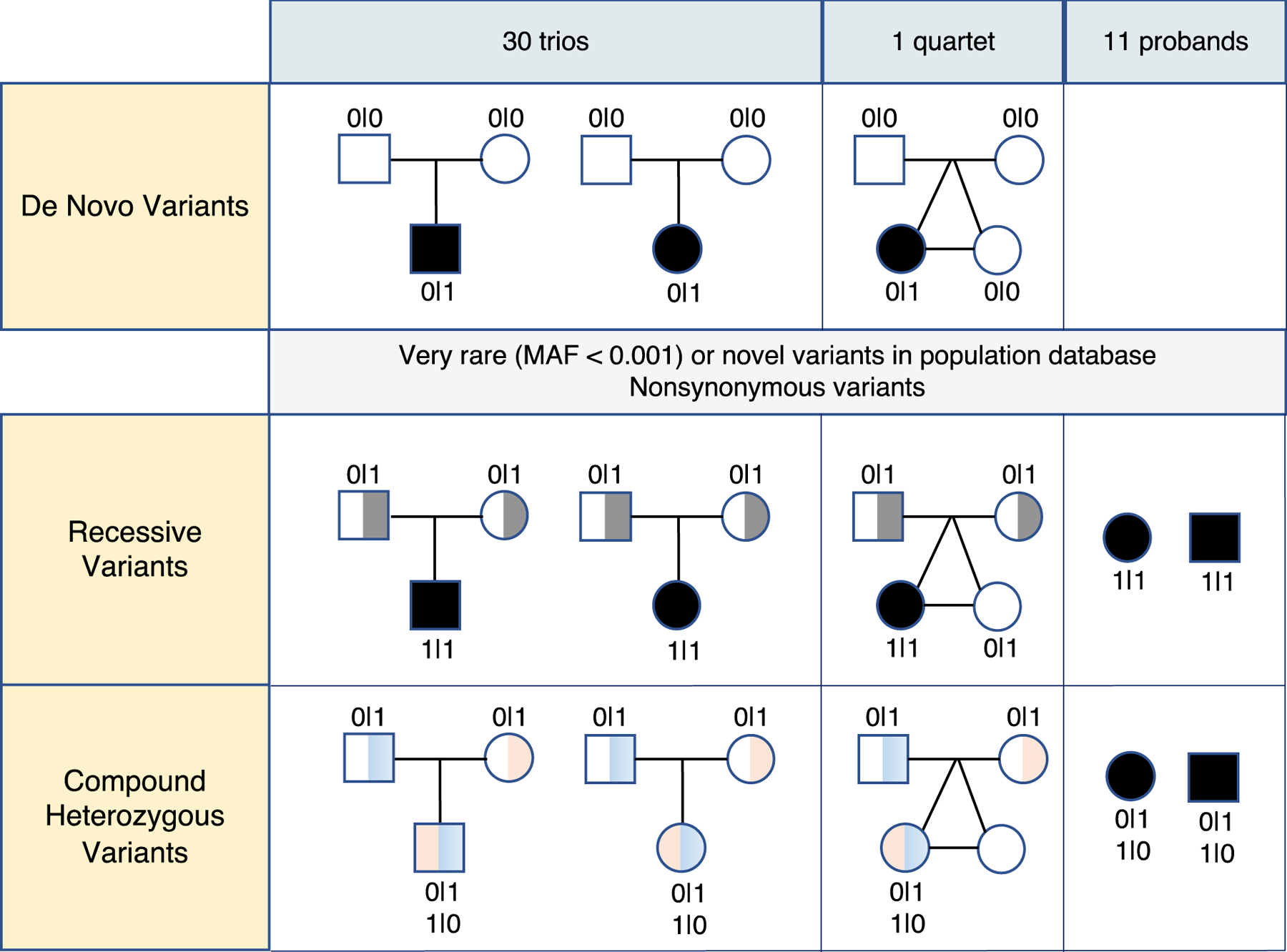
Methods: We enrolled patients diagnosed with OMAS before the age of 18 years at a pediatric neuroimmunology clinic in Boston, United States, using the 2004 Genoa Criteria. Whole genome sequencing was conducted for the patients and their biological parents in all cases, with one case including an unaffected twin sibling.
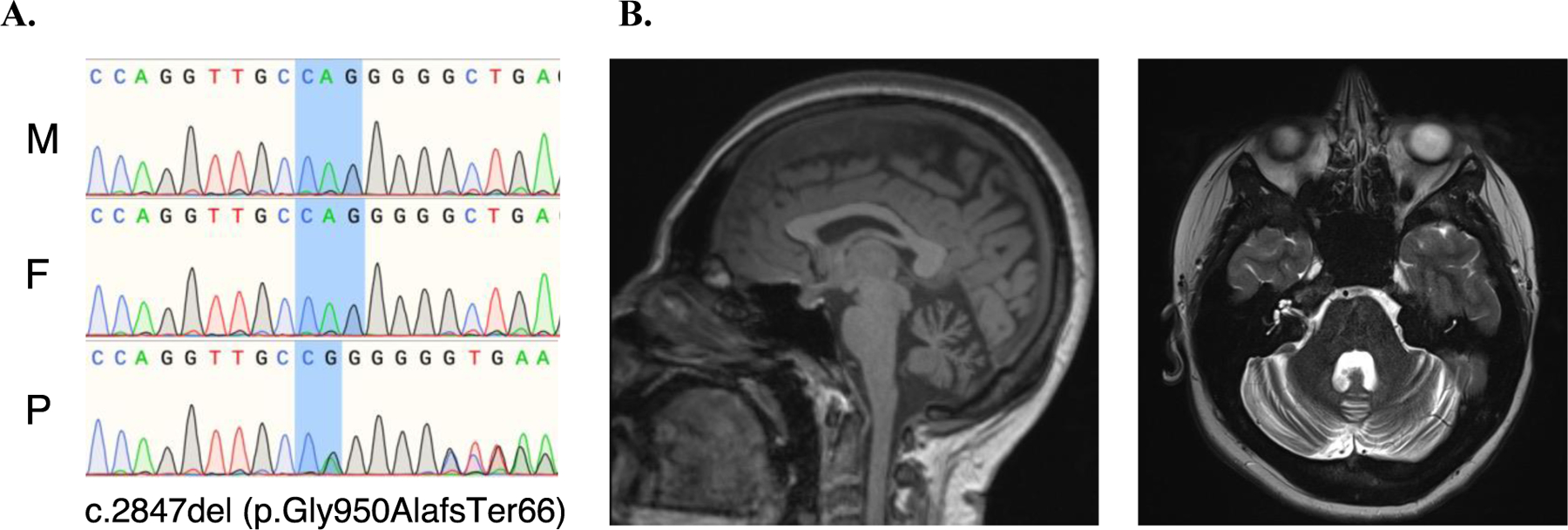
Results: De novo germline variants (DNVs) in probands were identified and validated and analyses of structural variants, recessive variants in neuroimmune-associated genes, and high-resolution human leukocyte antigen (HLA) typing were performed. Our study included 42 patients, 23 of whom had neuroblastoma. We found 12 confirmed DNVs in protein-coding regions in nine patients (29.0% of 31 from 30 trios and 1 quartet). Ten patients (23.8% of 42) had rare homozygous or compound heterozygous variants known to alter protein function, affecting 11 genes. Notably, the major histocompatibility complex, class II, DR beta 1 (HLA-DRB1) ∗01 allele was observed in 27 out of 84 (32.1%) alleles in the patients, significantly higher than that in the general population (chi-square test, P < 0.0001). In one case, a potential genetic modifier of OMAS with severe cerebellar atrophy was identified, associated with a protein-truncating DNV in the CACNA2D2 gene.
Conclusions: This first genome sequencing study reveals potential genetic contributors to OMAS, implicating polygenic predisposition-with HLA-DRB1∗01 as a possible factor-combined with nongenetic risk factors like neuroblastoma.
Keywords: Compound heterozygous; De novo germline variants; Linked-reads genome sequencing; Opsoclonus-myoclonus-ataxia syndrome; Recessive.
Copyright © 2025 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest None.
Figures
References
-
- Gorman MP. Update on diagnosis, treatment, and prognosis in opsoclonus-myoclonus-ataxia syndrome. Curr Opin Pediatr 2010;22:745–750. - PubMed
-
- Gambini C, Conte M, Bernini G, et al. Neuroblastic tumors associated with opsoclonus-myoclonus syndrome: histological, immunohistochemical and molecular features of 15 Italian cases. Virchows Arch 2003;442:555–562. - PubMed
-
- Torres-Vega E, Duran-Moreno M, Sanchez Del Pino M, et al. Immunoproteomic studies on paediatric opsoclonus-myoclonus associated with neuroblastoma. J Neuroimmunol 2016;297:98–102. - PubMed
-
- Graus F, Dalmau J. Paraneoplastic neurological syndromes in the era of immune-checkpoint inhibitors. Nat Rev Clin Oncol 2019;16:535–548. - PubMed
-
- Anand G, Bridge H, Rackstraw P, et al. Cerebellar and cortical abnormalities in paediatric opsoclonus-myoclonus syndrome. Dev Med Child Neurol 2015;57:265–272. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
