

Diagnostic prediction of neonatal hyperbilirubinemia combined with germinal matrix-intraventricular hemorrhage based on cranial ultrasound hemodynamics: a retrospective case-control study
- PMID: 41020227
- PMCID: PMC12460360
- DOI: 10.3389/fmed.2025.1606892
Diagnostic prediction of neonatal hyperbilirubinemia combined with germinal matrix-intraventricular hemorrhage based on cranial ultrasound hemodynamics: a retrospective case-control study
Abstract
Objective: To study the diagnostic prediction of cranial ultrasound hemodynamics in children with neonatal hyperbilirubinemia combined with germinal matrix-intraventricular hemorrhage (GMH-IVH).
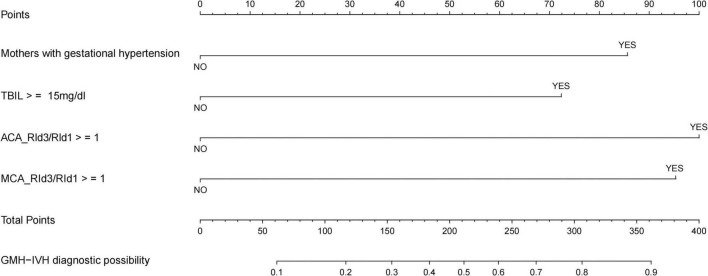
Methods: We included 148 hyperbilirubinemic neonates who underwent cranial ultrasound to obtain hemodynamic parameter indexes, and constructed a nomogram visual prediction model through unifactorial and multifactorial analyses to study the role of cranial ultrasound hemodynamic parameters in the diagnostic prediction of neonatal hyperbilirubinemia combined with GMH-IVH.
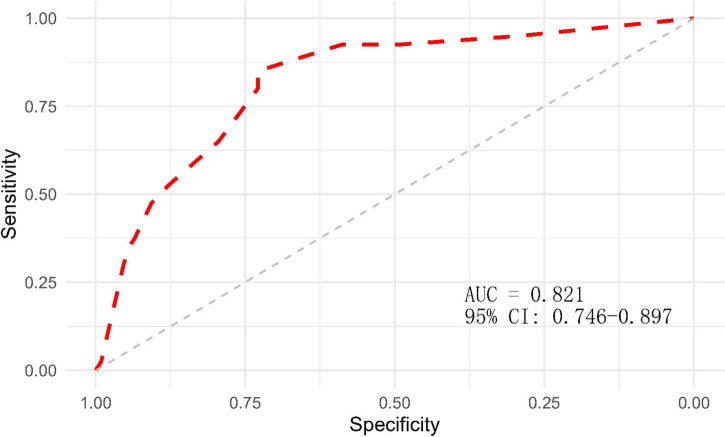
Results: A total of 148 patients eligible for enrollment were included in this study, of which 40 children developed GMH-IVH, with an incidence rate of 27.03%. Multifactorial logistic stepwise regression analysis showed that mothers suffering from gestational hypertension, total bilirubin ≥15 mg/dl, anterior cerebral artery third day to first day resistance index ratio of ≥1, and middle cerebral artery third day to first day resistance index ratio of ≥1 were the independent risk factors for the development of GMH-IVH in neonatal hyperbilirubinemic infants (P < 0.05); and ROC analysis showed that the area under the ROC curve (AUC) of the prediction model was 0.821 (95% CI: 0.746-0.897, P < 0.001), indicating good predictive efficacy of the model (discrimination), and the Hosmer-Lemeshow test (χ2 = 7.779, P = 0.255) and the calibration curve showed that the model had a good goodness-of-fit (calibration). The predictive model was visualized by plotting nomogram.
Conclusion: Craniocerebral ultrasound hemodynamics-related parameters combined with clinical features to construct a predictive model for early and effective prediction of the occurrence and prognosis of GMH-IVH in neonates with hyperbilirubinemia.
Keywords: cranial ultrasound hemodynamics; germinal matrix-intraventricular hemorrhage; neonatal hyperbilirubinemia; nomogram; prediction.
Copyright © 2025 Ye, Chen, Wu, Lin and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Desai S, Athalye-Jape G, Madhala S, Tee W, Sharp M, Nathan E, et al. Comparison of papile versus laterality-based Al-Abdi system to predict neurodevelopmental impairment in extreme preterm infants after severe germinal matrix hemorrhage-intraventricular hemorrhage: a retrospective comparative observational study. AJNR Am J Neuroradiol. (2022) 43:486–92. 10.3174/ajnr.A7434 - DOI - PMC - PubMed
-
- Fernandez de Gamarra-Oca L, Zubiaurre-Elorza L, Junque C, Solana E, Soria-Pastor S, Vazquez E, et al. Reduced hippocampal subfield volumes and memory performance in preterm children with and without germinal matrix-intraventricular hemorrhage. Sci Rep. (2021) 11:2420. 10.1038/s41598-021-81802-7 - DOI - PMC - PubMed