

Tumor-specific major histocompatibility-II expression predicts pathological complete response to atezolizumab combined to chemotherapy in triple-negative breast cancer
- PMID: 41022779
- PMCID: PMC12480687
- DOI: 10.1038/s41523-025-00828-6
Tumor-specific major histocompatibility-II expression predicts pathological complete response to atezolizumab combined to chemotherapy in triple-negative breast cancer
Abstract
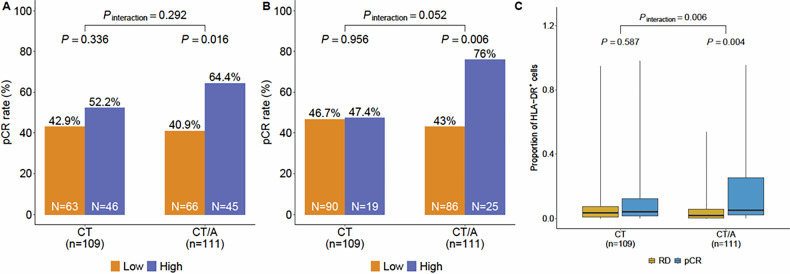
Adding immune checkpoint inhibitors to neoadjuvant chemotherapy improves outcomes in early-stage triple-negative breast cancer (TNBC), but a fraction of patients derive benefit. Tumor-specific MHC-II (tsMHC-II) expression has been shown to be a predictive biomarker of pathological complete response (pCR) to neoadjuvant chemo-immunotherapy in early-stage TNBC. We performed biomarker analysis of the phase III NeoTRIP trial where patients were randomized to neoadjuvant carboplatin and nab-paclitaxel±atezolizumab. Imaging mass cytometry was used to assess tsMHC-II expression in tumor samples. TsMHC-II positivity was predefined as ≥5% of tumor cells expressing MHC-II, and at an 80th percentile exploratory cutoff. TsMHC-II positivity was associated with a higher pCR rate in the atezolizumab arm (OR:2.58; P = 0.016), but not in the chemotherapy-only arm (OR:1.37; P = 0.34) and these results were stronger using the exploratory cutoff. TsMHC-II expression is associated with improved response to neoadjuvant chemo-immunotherapy in early TNBC and could represent a clinically useful predictive biomarker for treatment personalization.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: J.M.B. receives research support from Genentech/Roche and Incyte Corporation, has received advisory board payments from AstraZeneca, Eli Lilly, and Mallinckrodt and is an inventor on patents regarding immunotherapy targets and biomarkers in cancer. L.P. has received consulting fees and honoraria for advisory board participation from Pfizer, Astra Zeneca, Merck, Bristol-Myers Squibb, Stemline-Menarini, BeiGene, Personalis, Natera, Agendia, Exact Sciences, Radionetics, and institutional research funding from Pfizer, AstraZeneca, Merck, Bristol Myers Squibb, and Menarini-Stemline. Stock options in Ataraxis.GB has received consulting fees from Seagen, Roche, AstraZeneca, MSD, Daiichi Sankyo, Menarini, Tethis and Gilead Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events: Roche, AstraZeneca, Daiichi Sankyo, Eli Lilly, MSD, Gilead, Seagen, Pfizer, Novartis, Takeda; Support for attending meetings and/or travel: Roche, Pfizer, MSD, Novartis, Daiichi Sankyo, AstraZeneca, Takeda, Gilead, Eli Lilly, Menarini; and Advisory Board fees from Helsinn, Pfizer, Roche, AstraZeneca, Eli Lilly, Novartis, MSD, Daiichi Sankyo, Gilead, Seagen, Menarini, Exact Science. L.L. has received consulting fee from Exact Sciences, Helsinn, AstraZeneca, Daiichi Sankyo; honoraria for speakers’ bureaus from Gilead, Exact Sciences, Helsinn, Lilly, AstraZeneca, Daiichi Sankyo; support for attending meetings from Lilly, Gilead, Accord, Helsinn, Roche; has served on Advisory Board for Lilly, Exact Sciences, AstraZeneca, Italfarmaco, Daiichi Sankyo, Accord, Pfizer, Gilead, Novartis.
Figures
References
-
- Schmid, P. et al. Pembrolizumab for early triple-negative breast cancer. N. Engl. J. Med.382, 810–821 (2020). - PubMed
-
- Schmid, P. et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N. Engl. J. Med.386, 556–567 (2022). - PubMed
-
- Bianchini, G., De Angelis, C., Licata, L. & Gianni, L. Treatment landscape of triple-negative breast cancer - expanded options, evolving needs. Nat. Rev. Clin. Oncol.19, 91–113 (2022). - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
