

Catecholaminergic nucleus integrity and Alzheimer's pathology, symptoms, and progression
- PMID: 41023472
- PMCID: PMC12479218
- DOI: 10.1002/alz.70749
Catecholaminergic nucleus integrity and Alzheimer's pathology, symptoms, and progression
Abstract
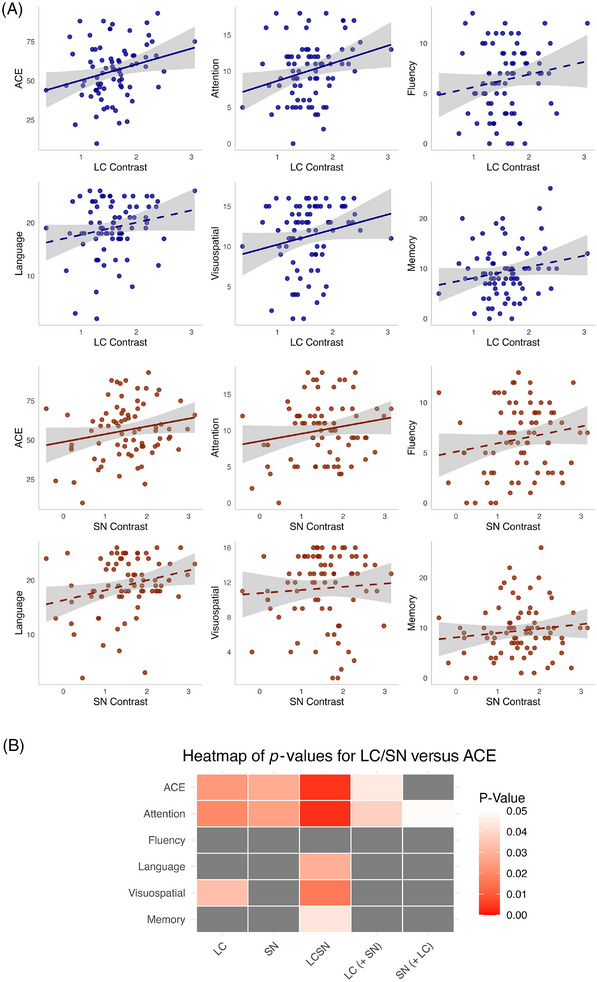
Background: The noradrenergic locus coeruleus (LC) accumulates pathology early in Alzheimer's disease (AD), with LC dysfunction contributing to symptoms and disease progression. We investigated LC and substantia nigra (SN) integrity in healthy controls and AD participants.
Methods: Ninety-three AD participants and 29 controls underwent neuromelanin magnetic resonance imaging. LC and SN contrast, reflecting nucleus integrity, related to cognitive and neuropsychiatric symptoms, as well as cognitive decline and atrophy rates.
Results: LC - but not SN - integrity was reduced in AD versus controls (b = -0.39, p = 0.001) and within AD was associated with global cognition (b = 8.53, p = 0.04) and neuropsychiatric symptoms, accounting for SN. An AD subgroup with reduced SN integrity had worse cognition. LC integrity predicted plasma phosphorylated tau protein 217 (b = -0.30, p = 0.03). Lower LC and SN integrities were both related to faster cognitive decline (LC: b = -4.74, p = 0.048; SN: b = -2.27, p = 0.03), accounting for one another.
Discussion: Catecholaminergic nucleus integrity plays an important role in AD. Both systems are relevant to cognitive performance and decline. LC, in particular, relates closely to symptoms, pathology, and rate of progression.
Highlights: In symptomatic AD, LC integrity reflects cortical AD pathology, measured by pTau217. LC integrity predicts cognitive function in AD, independent of cortical atrophy. LC and SN integrity independently relate to attentional performance. Symptoms of anxiety, depression, and apathy are associated with lower LC integrity. LC and SN relate to cognitive decline rate and left LC predicts atrophy rate.
Keywords: catecholamines; cognition; disease progression; dopamine; locus coeruleus; neuromelanin; neuropsychiatric symptoms; noradrenaline; norepinephrine; substantia nigra.
© 2025 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
Paresh A. Malhotra is lead for a NIHR‐funded trial with drug/placebo provided by Takeda Pharmaceuticals and sits on the Data Monitoring Committee for a trial carried out by Johnson & Johnson. He is vice chair of the Alzheimer's Society Research Strategy Council and NIHR Specialty Lead for Dementia and Neurodegeneration, Research Delivery Network. He is also an independent member of a data monitoring committee. All other authors have nothing to disclose. Author disclosures are available in the Supporting Information.
Figures






References
-
- Sara SJ. The locus coeruleus and noradrenergic modulation of cognition. Nat Rev Neurosci. 2009;10(3):211–223. - PubMed
-
- Berridge CW, Waterhouse BD. The locus coeruleus‐noradrenergic system: modulation of behavioral state and state‐dependent cognitive processes. Brain Res Rev. 2003;42(1):33–84. - PubMed
-
- Brunello N, Blier P, Judd LL, et al. Noradrenaline in mood and anxiety disorders: basic and clinical studies. Int Clin Psychopharmacol. 2003;18(4):191–202. - PubMed
-
- Weinshenker D. Long road to ruin: noradrenergic dysfunction in neurodegenerative disease. Trends Neurosci. 2018;41(4):211–223. http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D&med15&NEWS=N&AN... - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
