

Safety and efficacy of three-dimensional reconstruction technology-assisted percutaneous transhepatic biliary drainage: A meta-analysis
- PMID: 41024800
- PMCID: PMC12476638
- DOI: 10.4240/wjgs.v17.i9.105134
Safety and efficacy of three-dimensional reconstruction technology-assisted percutaneous transhepatic biliary drainage: A meta-analysis
Abstract
Background: Percutaneous transhepatic biliary drainage (PTBD) is one of the primary clinical treatment options for patients with obstructive jaundice. In recent years, PTBD assisted by three-dimensional (3D) reconstruction technology has been widely implemented, but its advantages over traditional methods remains inconclusive. Thus, a discussion is warranted.
Aim: To explore the safety and efficacy of 3D reconstruction technology-assisted PTBD.
Methods: We systematically searched the databases including the Cochrane Library, PubMed, EMBASE, Web of Science and China National Knowledge Infrastructure. The search period extended from the establishment of each database to November, 2024. We screened the literature according to predefined inclusion and exclusion criteria, assessed the quality of the studies, and extracted data. Meta-analysis was performed using Revman 5.4.1 software.
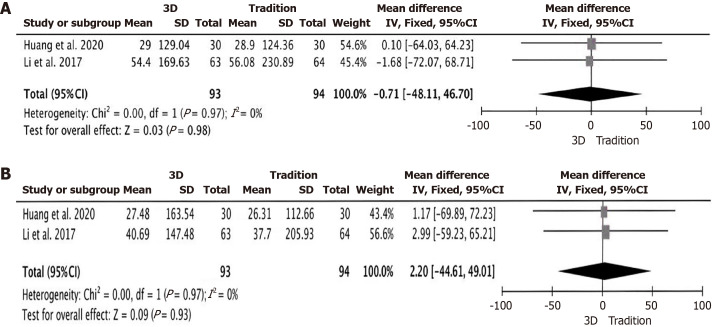
Results: A total of 15 studies were included, involving 1434 patients. The results of the meta-analysis showed that compared with the traditional group, the overall post-operative complications rate in the 3D reconstruction technology group was significantly lower [odds ratio = 0.25; 95% confidence interval (CI): 0.17-0.36, P < 0.00001]. The overall puncture success rate in the 3D reconstruction group was better than those in the traditional group (odds ratio = 3.61; 95%CI: 1.98-6.55, P < 0.0001). However, there was no significant difference between the two groups in the reduction levels of postoperative total bilirubin (mean difference = -1.38; 95%CI: -3.29 to 0.53, P = 0.16). Subgroup analysis were conducted on the surgery time according to guidance stages of the 3D reconstruction, 3D reconstruction imaging modalities, and types of studies. The results were stable, with no significant changes observed.
Conclusion: 3D reconstruction technology significantly improves the puncture success rate and safety of PTBD. However, it has no significant advantage in bile drainage effectiveness. Continued research is warranted to further explore its clinical value and optimize its application.
Keywords: Complications; Liver function; Obstructive jaundice; Percutaneous transhepatic biliary drainage; Three-dimensional reconstruction technology.
©The Author(s) 2025. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures





References
-
- Jin H, Pang Q, Liu H, Li Z, Wang Y, Lu Y, Zhou L, Pan H, Huang W. Prognostic value of inflammation-based markers in patients with recurrent malignant obstructive jaundice treated by reimplantation of biliary metal stents: A retrospective observational study. Medicine (Baltimore) 2017;96:e5895. - PMC - PubMed
-
- Pavlidis ET, Pavlidis TE. Pathophysiological consequences of obstructive jaundice and perioperative management. Hepatobiliary Pancreat Dis Int. 2018;17:17–21. - PubMed
-
- Yang F, Jin C, Zou C, Di Y, Hao S, Huang H, Warshaw AL, Fu D. Delaying surgery after preoperative biliary drainage does not increase surgical morbidity after pancreaticoduodenectomy. Surgery. 2019;166:1004–1010. - PubMed
-
- Cao J, Wang Z, Cai H, Zhang J, Yue Y, Liu X, Zhang D. Effect of PTCD-based biliary stent placement combined with 125I particle intracavitary irradiation in treating pancreatic head cancer. J BUON. 2020;25:1056–1062. - PubMed
LinkOut - more resources
Full Text Sources
