

A case series of OMI: time for revisiting STEMI/NSTEMI ECG criteria
- PMID: 41026420
- PMCID: PMC12484458
- DOI: 10.1186/s43044-025-00688-2
A case series of OMI: time for revisiting STEMI/NSTEMI ECG criteria
Abstract
Background: The current STEMI criteria fail to detect roughly one-third of occlusive MI (OMI). STEMI criteria demonstrated only a sensitivity of around 21% for OMI. Compared to STEMI, patients with NSTEMI-OMI have higher short-term and long-term all-cause mortality and longer reperfusion delays. This case series presents three NSTEMI patients with OMI and a delayed reperfusion strategy.
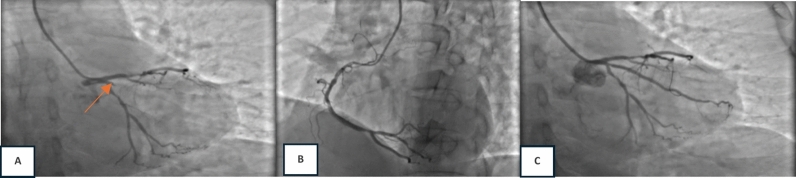
Case presentation: We present three cases of patients initially diagnosed with NSTEMI who were later found to have occlusive myocardial infarction (OMI) based on angiographic findings, all of whom underwent delayed reperfusion strategies. The first two cases shared similar clinical profiles, presenting with typical infarct angina, elevated cardiac enzymes, and regional wall motion abnormalities on echocardiography. Their electrocardiograms showed bifascicular blocks, right bundle branch block (RBBB) with left posterior fascicular block (LPFB) in the first case, and RBBB with left anterior fascicular block (LAFB) in the second. Both were classified as high-risk NSTEMI and scheduled for an early invasive approach. Angiography revealed total occlusions in the OM1 and left main arteries, respectively. In the third case, the patient presented with new-onset angina and elevated cardiac biomarkers, but without ECG features fulfilling STEMI or high-risk OMI criteria. However, due to persistent chest pain despite initial treatment in the emergency department, an immediate invasive strategy was pursued. Coronary angiography revealed a total occlusion in the proximal left anterior descending (LAD) artery.
Conclusions: These three cases underscore the diagnostic challenge of identifying occlusive myocardial infarction (OMI) in patients presenting with acute coronary syndrome (ACS) when relying exclusively on traditional STEMI criteria. They emphasize the need to recognize alternative ECG markers indicative of acute coronary occlusion, as failure to do so may result in delayed reperfusion and subsequently worse clinical outcomes compared to patients who receive timely intervention based on prompt STEMI recognition.
Keywords: Delayed reperfusion; OMI/NOMI; STEMI/NSTEMI.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All procedures followed in this report were by the ethical standard of the Declaration of Helsinki 2013. The subjects of the patient for this case report is under the ethical clearance registry. The Name of the ethics committee is the Research Ethics Committee of the National Cardiovascular Center Harapan Kita, The reference number: DP.04.03/KEP056/EC023/2024. Consent for publication: Written informed consent was obtained from the patient for inclusion in this case report, ensuring that no identifying information has been disclosed. Competing interests: The authors declare no competing interests.
Figures





References
-
- Nunes J, Scheffer MK, Correia BP, Franchini KG, Felicioni SP, Fuziy M (2024) Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Int J Cardiol 402:131889–131899 - PubMed
LinkOut - more resources
Full Text Sources