

Catheter-assisted sealing technique for spontaneous cerebrospinal fluid leaks: A novel neurointerventional treatment of spontaneous cerebrospinal fluid leak beyond cerebrospinal fluid-venous fistula
- PMID: 41026952
- PMCID: PMC12484073
- DOI: 10.1177/15910199251376452
Catheter-assisted sealing technique for spontaneous cerebrospinal fluid leaks: A novel neurointerventional treatment of spontaneous cerebrospinal fluid leak beyond cerebrospinal fluid-venous fistula
Abstract
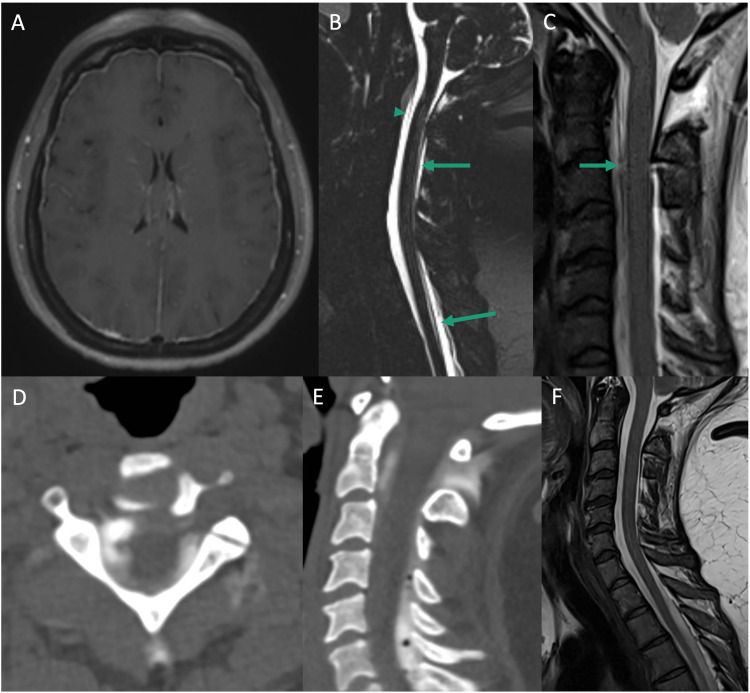
BackgroundSpontaneous intracranial hypotension (SIH) is a severe condition caused by cerebrospinal fluid (CSF) leaks, leading to headaches and neurological impairments. Traditional epidural blood patch treatment is often ineffective, especially in refractory cases without a source leak identified. This study introduces and evaluates the Catheter-Assisted Sealing Technique (CAST), a novel neurointerventional approach for refractory SIH. CAST involves targeted or diffuse delivery of fibrin glue into the epidural space to repair CSF leaks.MethodsA retrospective case series of ten patients with refractory SIH underwent CAST using a fluoroscopy-guided epidural catheter approach. Clinical symptom resolution and follow-up MRI findings were assessed.ResultsNine of 10 patients achieved complete headache resolution and associated symptom relief. One patient experienced significant improvement without complete relief. Follow-up MRI showed resolution of pachymeningeal enhancement in all patients. One patient required repeat procedures for recurrent symptoms. No neurological injury or spinal cord compression occurred, with the only complication being transient femoral nerve palsy due to positioning that resolved within four months.ConclusionCAST is a promising, minimally invasive alternative for refractory SIH. It enables targeted or diffuse fibrin sealant application, providing a seemingly effective leak closure even in cases of occult or multifocal leaks. Early results show high success and safety rates, but larger cohorts and extended follow-up are needed to validate it as a standard treatment.
Keywords: CSF leak; Spine; epidural blood patch; intracranial hypotension.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures





References
-
- Schievink WI, Maya MM, Moser FG, et al. Incidence of spontaneous intracranial hypotension in a community: Beverly Hills, California, 2006–2020. Cephalalgia 2022; 42: 312–316. - PubMed
-
- Liaquat MT, Jain S. Spontaneous intracranial hypotension. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. http://www.ncbi.nlm.nih.gov/books/NBK559066/ (2024, accessed 9 August 2024).
-
- Schievink WI. Misdiagnosis of spontaneous intracranial hypotension. Arch Neurol 2003; 60: 1713–1718. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
