

Hypotension prediction index smart alerts and trends to improve compliance with goal-directed hemodynamic therapy: a feasibility study
- PMID: 41029588
- PMCID: PMC12482379
- DOI: 10.1186/s12871-025-03336-z
Hypotension prediction index smart alerts and trends to improve compliance with goal-directed hemodynamic therapy: a feasibility study
Abstract
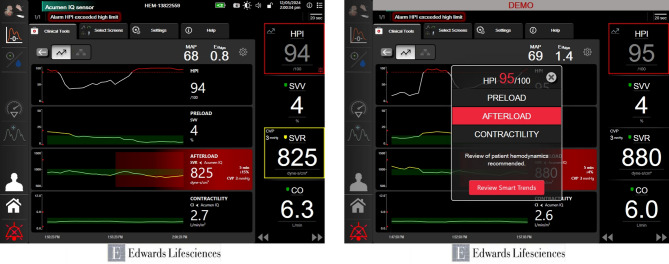
Background: Goal-directed hemodynamic therapy (GDHT) and Hypotension Prediction Index (HPI, Edwards Lifesciences, Irvine, CA) technology are used to improve post-operative patient outcomes. Trials evaluating GDHT are frequently limited by poor algorithm compliance. The Acumen HPI Software incorporates smart trends and alerts that highlight the probable mechanism(s) of hypotension and facilitate compliance with the GDHT algorithm. We hypothesized that prompts from the Acumen HPI Smart Alerts would improve compliance to a GDHT algorithm during moderate-to-high-risk elective noncardiac surgery.
Methods: This IRB-approved, multicenter, mixed-methods, single-arm feasibility trial included adults undergoing elective, moderate-to-high-risk noncardiac surgery requiring intra-arterial blood pressure monitoring. The HPI-guided GDHT algorithm included actionable trends at HPI > 50 and automated HPI Smart Alert notifications at HPI ≥ 85, displaying the most likely hypotension mechanism(s). The primary outcome was the proportion of HPI notifications resulting in timely algorithm-concordant interventions. The sample size was estimated to achieve a true compliance rate of at least 75% with a 95% confidence level above 60%.
Results: A total of 122 subjects were included. The enrollment among centers was balanced. The overall compliance rate was 77.1% (95% CI: 74.5-79.6%). The median area under the curve, time-weighted average, and minutes of hypotension below 65 mmHg were 8.8 (0.3, 33.7) mmHg*min, 0.0 (0.0, 0.1) mmHg, and 2.9 (0.4, 8.7) minutes, respectively.
Conclusions: This study demonstrated the potential for HPI Smart Alerts to improve compliance with an intraoperative GDHT algorithm in adults undergoing moderate to high-risk non-cardiac surgery. A low burden of intra-operative hypotension was observed, suggesting potential decreases in other associated adverse outcomes. Larger-scale randomized studies are warranted.
Trial registration: This trial was retrospectively registered at ClinicalTrials.gov on 14 July 2023 (NCT05957406).
Keywords: Feasibility studies; Goal-directed hemodynamic therapy; Hypotension; Hypotension prediction index.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was conducted in accordance with the principles of the Declaration of Helsinki. It was approved by the WIRB-Copernicus Group (WCG IRB) in addition to each individual study site’s IRB. Written informed consent was obtained utilizing the IRB-approved consent form before subjects underwent any study procedures. Each candidate was given time to discuss study participation and have questions or concerns addressed by study personnel. All consent procedures were conducted in a manner that was consistent with applicable regulations and followed Good Clinical Practice (GCP). Consent for publication: Not applicable. Competing interests: All authors received travel and institutional financial support from Edwards Lifesciences, the sponsor of this study, for study-related activities. Dr. Guerra-Londono has received consulting honoraria from Edwards Lifesciences, previous institutional research funding from GE Healthcare for research unrelated to the topic of the manuscript, and ongoing institutional re-search funding from Vena Vitals. Dr. Fleming has received support for contracted research from Tsumera Pharmaceuticals, Masimo, Inc., Rostrum Medical Innovations and Edwards Lifesciences and honoraria from Edwards Lifesciences for invited presentations. Dr. Kumar has received research funding from Edwards Lifesciences, Hemosonics, Haisko Pharmaceu-ticals, Apple, and the Patient Centered Outcomes Research Institute (PCORI). Dr. Khanna consults for Medtronic, Edwards Lifesciences, Philips Research North America, GE Healthcare, Potrero Medical, Sentinel Medical, Retia Medical, Nihon-Kohden USA, Caretaker Medical, TNO, Bayer Corporation, Fifth Eye Inc., Renibus Therapeutics, Pharmazz Inc., AOP, Viatris, Innoviva Specialty Therapeutics and Zynex Medical. Dr. Khanna has ownership inter-ests with BrainX LLC. Dr. Treggiari reports research support from the National Institutes of Health (NIH). Dr. Dunkman, Dr. Hand, Dr. Davis, Dr. Domino, and Dr. Yang report no addi-tional conflicts besides those reported above for all authors regarding study-related activities.
Figures

References
-
- Kaufmann T, Clement RP, Scheeren TWL, Saugel B, Keus F, van der Horst ICC. Perioperative goal-directed therapy: a systematic review without meta-analysis. Acta Anaesthesiol Scand. 2018;62(10):1340–55. - PubMed
-
- Sessler DI, Bloomstone JA, Aronson S, Berry C, Gan TJ, Kellum JA, et al. Perioperative quality initiative consensus statement on intraoperative blood pressure, risk and outcomes for elective surgery. Br J Anaesth. 2019;122(5):563–74. - PubMed
-
- Maheshwari K, Shimada T, Yang D, Khanna S, Cywinski JB, Irefin SA, et al. Hypotension prediction index for prevention of hypotension during Moderate- to High-risk noncardiac surgery. Anesthesiology. 2020;133(6):1214–22. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
