

Multiple sclerosis: molecular pathogenesis and therapeutic intervention
- PMID: 41034190
- PMCID: PMC12488951
- DOI: 10.1038/s41392-025-02415-4
Multiple sclerosis: molecular pathogenesis and therapeutic intervention
Abstract
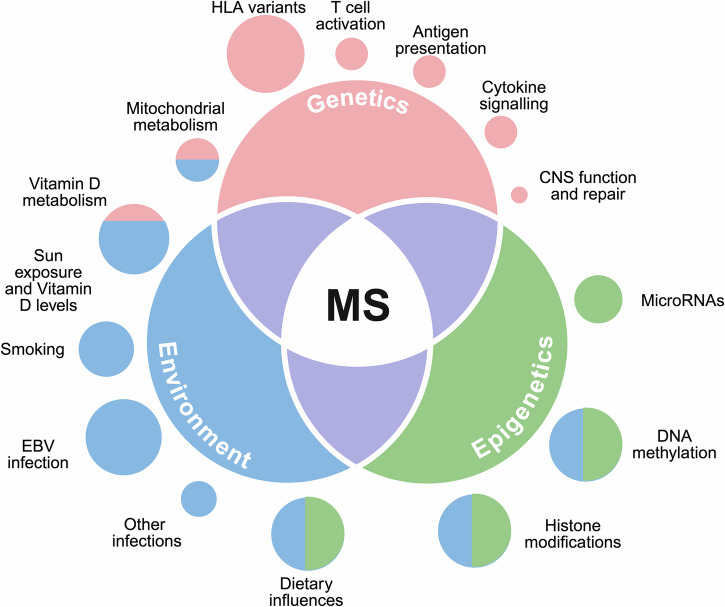
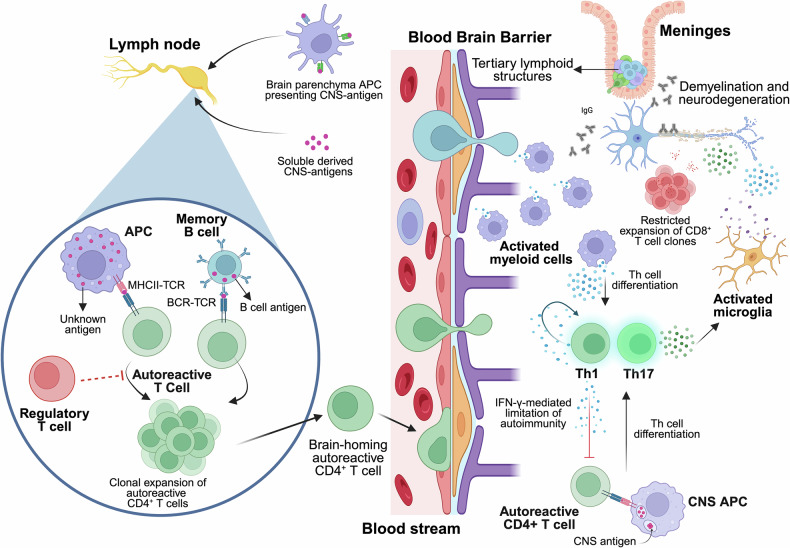
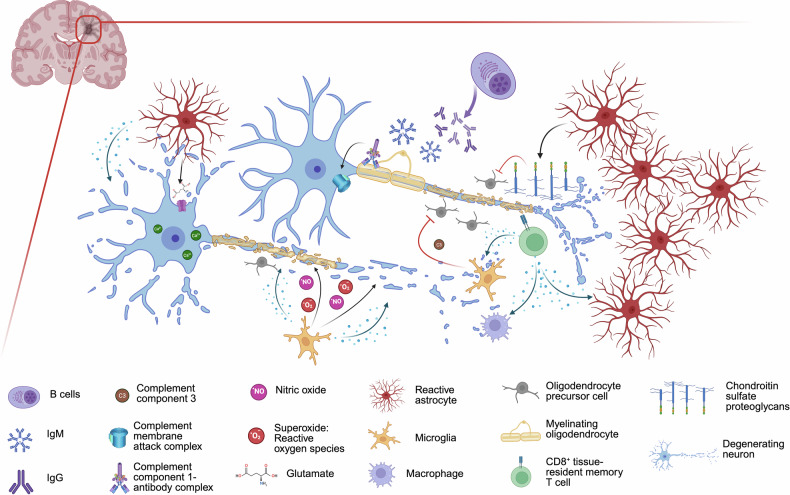
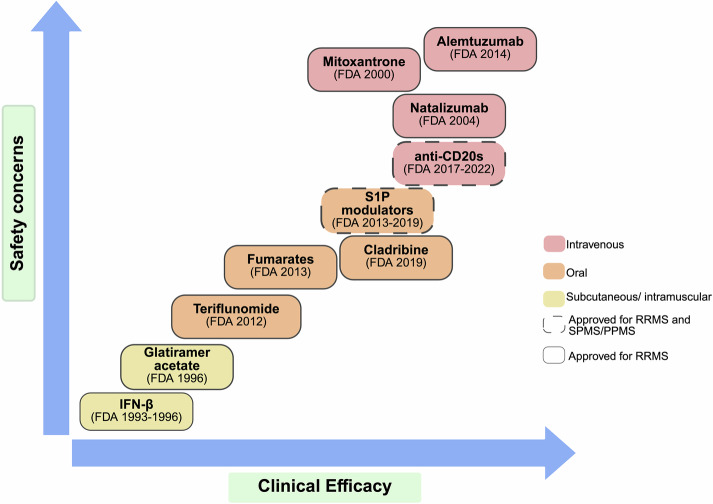
Multiple sclerosis is a chronic immune-mediated disorder of the central nervous system characterized by demyelination, axonal loss, and neuroinflammation, culminating in progressive neurological disability. Despite significant advances in understanding its immunopathogenesis, current immunotherapies remain limited in their ability to halt disease progression, making multiple sclerosis incurable and highlighting the critical need for novel therapeutic strategies. Antigen-specific immunotherapy represents a groundbreaking approach that aims to restore immune tolerance to myelin-derived antigens while preserving the protective functions of the immune system. Unlike broad immunosuppressive strategies, antigen-specific immunotherapy offers the potential for highly targeted modulation of pathogenic immune responses, reducing off-target effects and enhancing safety profiles. Over the last two decades, preclinical studies and clinical trials have explored diverse antigen-specific immunotherapy modalities, ranging from peptide-based vaccines to nanoparticle platforms, each aimed at achieving durable tolerance in multiple sclerosis. This review provides a comprehensive overview of multiple sclerosis, covering its etiology, clinical features, pathogenesis, pathology, and current therapeutic approaches. Thus, it delves into the current state of antigen-specific immunotherapy research, critically examining its successes and limitations while addressing the translational challenges that must be overcome to realize its therapeutic potential. By integrating insights from immunology, biotechnology, and translational medicine, we propose directions for advancing antigen-specific approaches in the quest for transformative multiple sclerosis therapies.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: I.B., A.H., and A.C.C. have nothing to disclose. J.V.A. has received grants from Instituto de Salud Carlos III, Spain; FI21/00282. H.E. and C.E. hold a patent related to liposome immunotherapy for autoimmune diseases, licensed to Ahead Therapeuthics, SL. X.M. has received speaking honoraria and travel expenses for scientific meetings; has been a steering committee member of clinical trials; or has participated in advisory boards of clinical trials in recent years, such as Abbvie, Actelion, Alexion, Biogen, Bristol-Myers Squibb/Celgene, EMD Serono, Genzyme, Hoffmann-La Roche, Immunic, Janssen Pharmaceuticals, Medday, Merck, Mylan, Nervgen, Novartis, Sandoz, Sanofi-Genzyme, Teva Pharmaceutical, TG Therapeutics, Excemed, MSIF and NMSS.
Figures

References
-
- Compston, A. & Coles, A. Multiple sclerosis. Lancet359, 1221–1231 (2002). - PubMed
-
- Jakimovski, D. et al. Multiple sclerosis. Lancet403, 183–202 (2024). - PubMed
-
- Simpson, S. Jr. et al. Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J. Neurol. Neurosurg. Psychiatry82, 1132–1141 (2011). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
