Pharmacogenomic synthetic lethal screens reveal hidden vulnerabilities and new therapeutic approaches for treatment of NF1-associated tumors
- PMID: 41036607
- PMCID: PMC12668261
- DOI: 10.1158/1535-7163.MCT-24-1053
Pharmacogenomic synthetic lethal screens reveal hidden vulnerabilities and new therapeutic approaches for treatment of NF1-associated tumors
Abstract
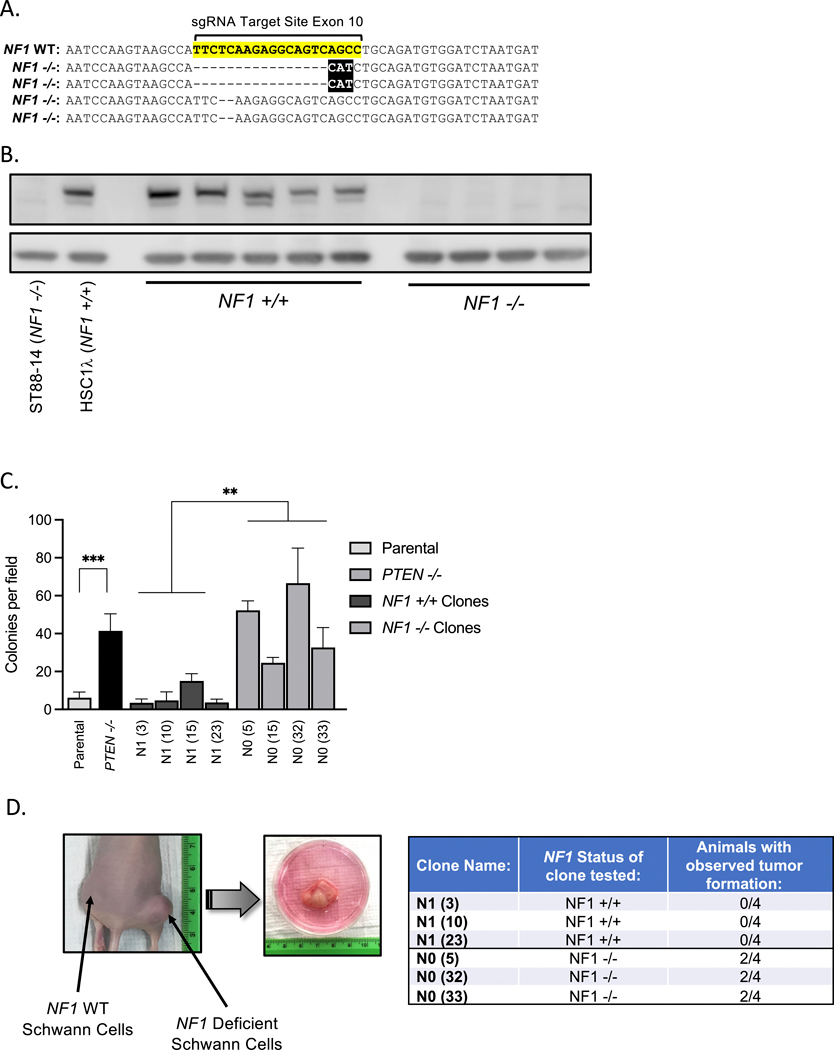
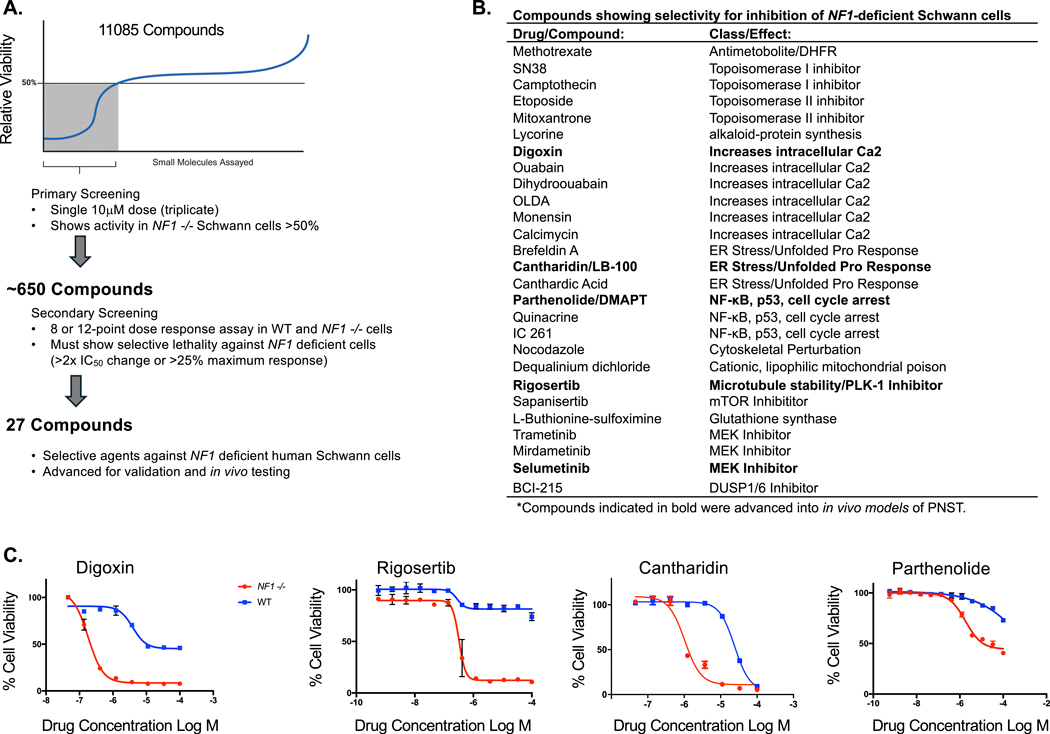
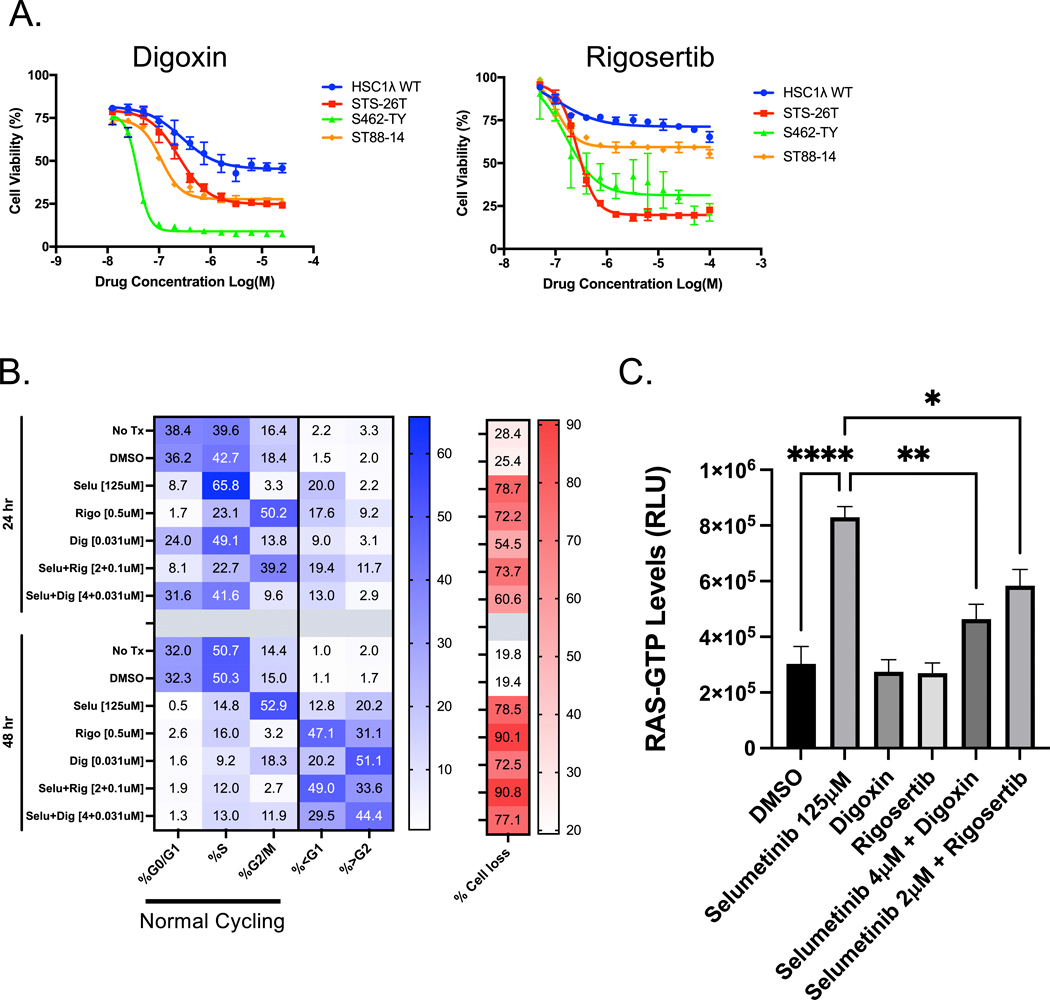
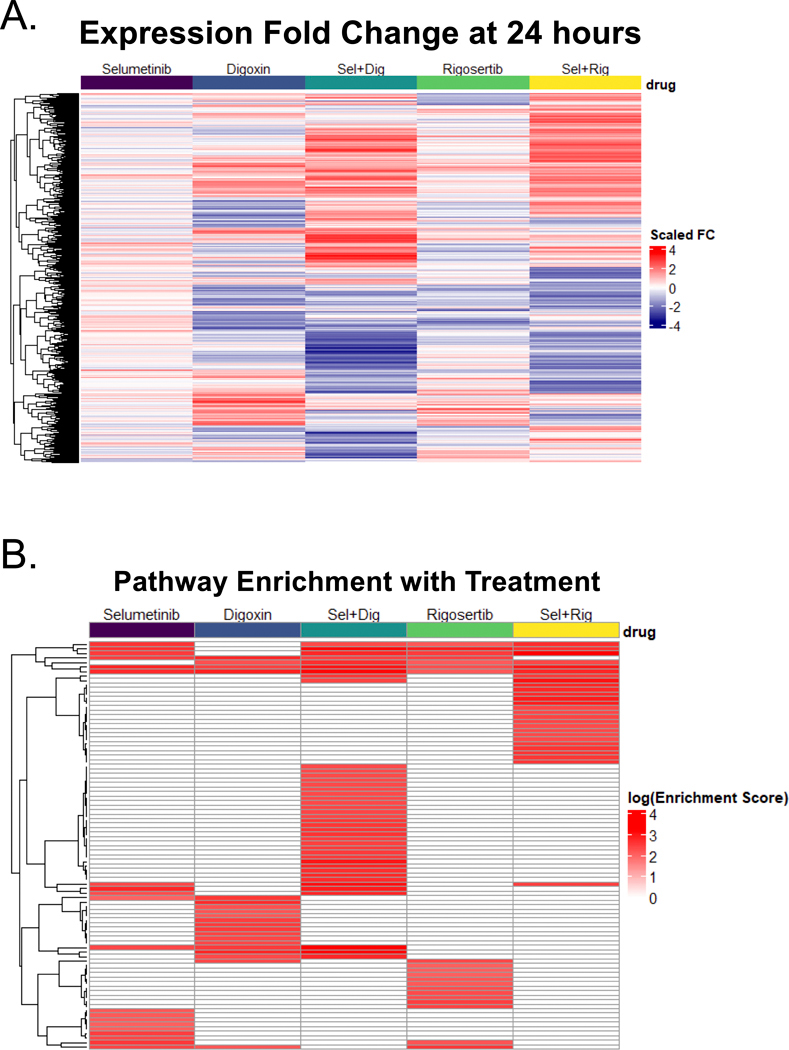
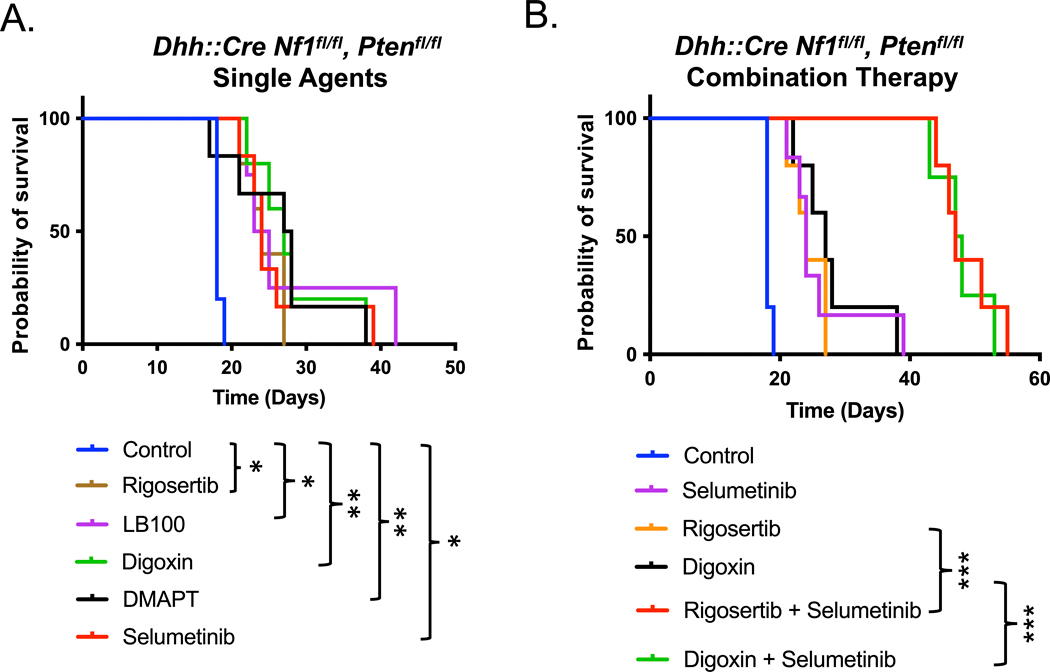
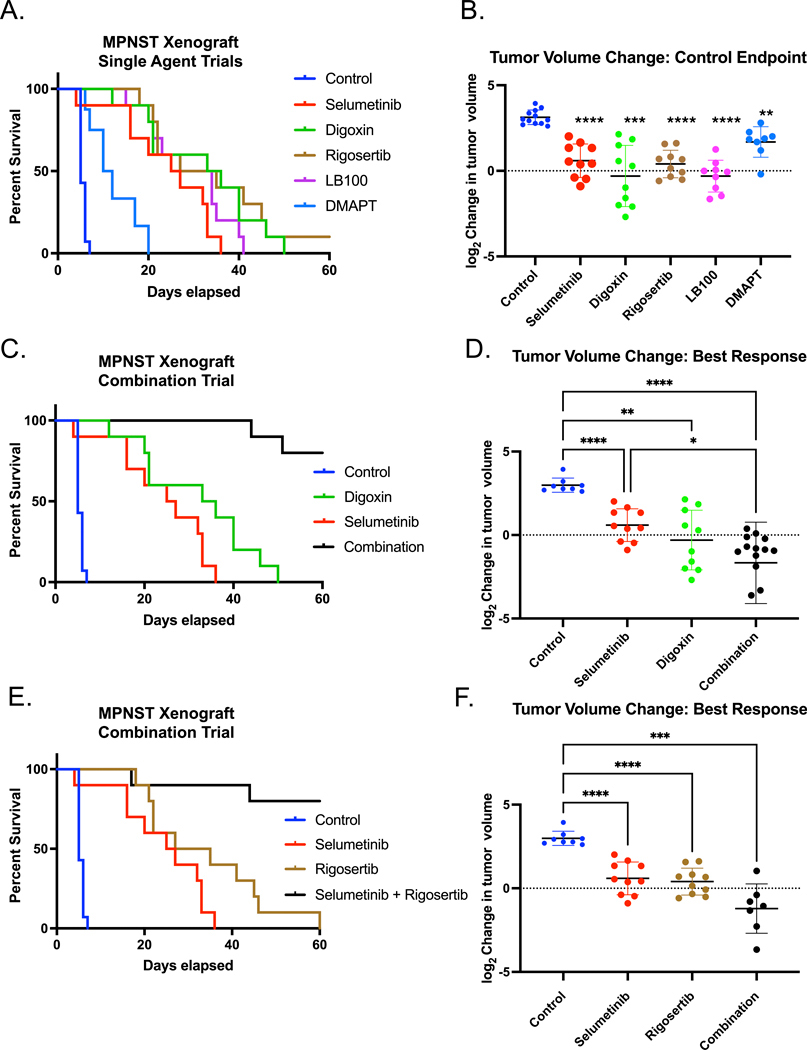
Neurofibromatosis Type 1 (NF1) is a common cancer predisposition syndrome caused by heterozygous loss of function mutations in the tumor suppressor gene NF1. Individuals with NF1 develop benign tumors of the peripheral nervous system (neurofibromas), originating from the Schwann cell linage after somatic loss of the wild-type NF1 allele, some of which progress further to malignant peripheral nerve sheath tumors (MPNST). There is only one FDA-approved targeted therapy for symptomatic plexiform neurofibromas and none approved for MPNST. The genetic basis of NF1 syndrome makes associated tumors ideal for using synthetic drug sensitivity approaches to uncover therapeutic vulnerabilities. We developed a drug discovery pipeline to identify therapeutics for NF1-related tumors using isogeneic pairs of NF1-proficient and deficient immortalized human Schwann cells. We utilized these in a large-scale high throughput screen (HTS) for drugs that preferentially kill NF1-deficient cells, through which we identified 23 compounds capable of killing NF1-deficient Schwann cells with selectivity. Multiple hits from this screen clustered into classes defined by the method of action. Four clinically interesting drugs from these classes were tested in vivo using both a genetically engineered mouse model of high-grade peripheral nerve sheath tumors and human MPNST xenografts. All drugs tested showed single-agent efficacy in these models as well as significant synergy when used in combination with the MEK inhibitor Selumetinib. This HTS platform yielded novel therapeutically relevant compounds for the treatment of NF1-associated tumors and can serve as a tool to rapidly evaluate new compounds and combinations in the future.
Conflict of interest statement
Figures
Update of
-
Pharmacogenomic synthetic lethal screens reveal hidden vulnerabilities and new therapeutic approaches for treatment of NF1-associated tumors.bioRxiv [Preprint]. 2024 Nov 1:2024.03.25.585959. doi: 10.1101/2024.03.25.585959. bioRxiv. 2024. Update in: Mol Cancer Ther. 2025 Oct 2. doi: 10.1158/1535-7163.MCT-24-1053. PMID: 38585724 Free PMC article. Updated. Preprint.
References
-
- Riccardi VM. Neurofibromatosis: Phenotype, Natural History and Pathogenesis. Neurology 2000;55(2):325- doi 10.1212/wnl.55.2.325. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous