

What Is On the Horizon for the Diagnosis and Treatment of SCLC and Large Cell Neuroendocrine Cancer?
- PMID: 41041628
- PMCID: PMC12485632
- DOI: 10.1016/j.jtocrr.2025.100871
What Is On the Horizon for the Diagnosis and Treatment of SCLC and Large Cell Neuroendocrine Cancer?
Abstract
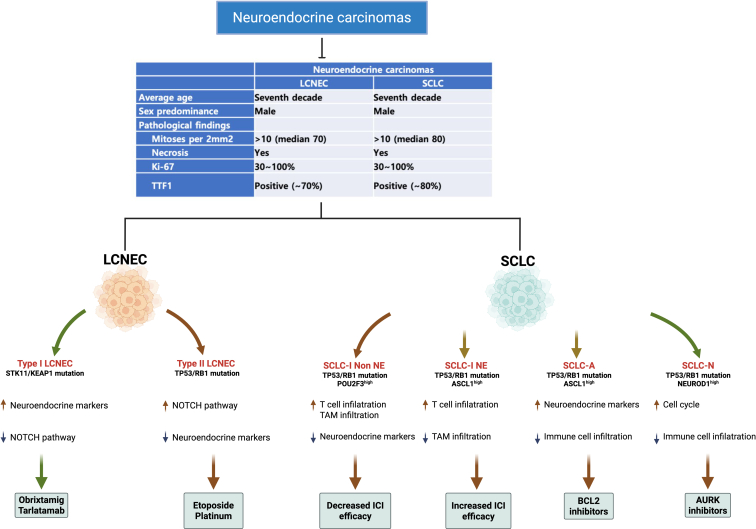
SCLC is a high-grade neuroendocrine malignancy associated with poor prognosis, comprising 15% of lung cancer cases globally. Advances in genetic profiling have revealed that SCLC is a molecularly heterogeneous disease, categorized into subtypes such as SCLC-A, SCLC-N, SCLC-P, and SCLC-I, on the basis of their neuroendocrine and immune-related characteristics. This heterogeneity underscores the need for tailored therapeutic strategies. Large cell neuroendocrine carcinoma (LCNEC) shares histologic and molecular similarities with SCLC but remains a distinct entity. LCNEC is categorized into two major subtypes: Type I, characterized by STK11 and KEAP1 mutations and a neuroendocrine phenotype, and Type II, defined by TP53 and RB1 alterations with higher proliferative indices. LCNEC's rarity and molecular diversity present challenges for standardized treatment, further highlighting the need for comparative research with SCLC. In this review, we highlight the genetic and clinicopathologic features of SCLC and LCNEC. Furthermore, we discuss emerging therapeutics and future directions in the treatment of SCLC and LCNEC.
Keywords: Diagnostics; Large cell neuroendocrine carcinoma; Novel therapies; Small cell lung cancer.
© 2025 by the International Association for the Study of Lung Cancer.
Conflict of interest statement
Dr. Soo receives research grants from 10.13039/100004325AstraZeneca, Boehringer Ingelheim, and 10.13039/100004319Pfizer; honoraria from AbbVie, Amgen, AnHeart, AstraZeneca, Bayer, BMS, Boehringer Ingelheim, Chugai, Daiichi Sankyo, GlaxoSmithKline (GSK), J INTS BIO, Janssen, Lily, Merck, Merck Serono, Novartis, Pfizer, Puma, Roche, Sanofi, Taiho, Takeda, Thermo Fisher, and Yuhan Corporation; and is a member of advisory board of AbbVie, Amgen, AnHeart, AstraZeneca, Bayer, BMS, Boehringer Ingelheim, Daiichi Sankyo, GSK, J INTS BIO, Janssen, Lily, Merck, Merck Serono, Novartis, Pfizer, Puma, Roche, Sanofi, Taiho, Takeda, Thermo Fisher, and Yuhan Corporation. Dr. Lim receives research grants from AstraZeneca, Boehringer Ingelheim, BioNTech, 10.13039/100015542GSK, 10.13039/100004337Roche, Hengrui, BridgeBio Therapeutics, Oscotec, Daichii-Sankyo, Johnson, and Johnson, J Ints Bio, Therapex, Yuhan, and MSD; and consulting fees from AstraZeneca, Boehringer Ingelheim, Lilly, Takeda, J Ints Bio, BMS, MSD, Oscotec, Merck, and Therapex. The remaining authors declare no conflict of interest.
Figures


References
-
- Gazdar A.F., Bunn P.A., Minna J.D. Small cell lung cancer: what we know, what we need to know and the path forward. Nat Rev Cancer. 2017;17:765. - PubMed
-
- Detterbeck F.C., Ostrowski M., Hoffmann H., et al. The International Association for the Study of Lung Cancer lung cancer staging project: proposals for revision of the classification of residual tumor after resection for the forthcoming (ninth) edition of the TNM classification of lung cancer. J Thorac Oncol. 2024;19:1052–1072. - PubMed
-
- Govindan R., Page N., Morgensztern D., et al. Changing epidemiology of small cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol. 2006;24:4539–4544. - PubMed
-
- Cittolin-Santos G.F., Knapp B., Ganesh B., et al. The changing landscape of small cell lung cancer. Cancer. 2024;130:2453–2461. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
