

Aspirin and healthy lifespan in older people: main outcome of the ASPREE-XT observational study
- PMID: 41043446
- PMCID: PMC12551462
- DOI: 10.1016/j.lanhl.2025.100764
Aspirin and healthy lifespan in older people: main outcome of the ASPREE-XT observational study
Abstract
Background: In the Aspirin in Reducing Events in the Elderly (ASPREE) clinical trial, low-dose aspirin was not associated with survival free of dementia and persistent physical disability (a measure of a healthy lifespan); however, there was a small increased risk of death. Given the long pre-clinical phase of many ageing conditions, we aimed to examine the legacy effect (post-trial) and the longer-term effect of aspirin versus placebo through extended follow-up in the ASPREE-XT observational study.
Methods: Between March 10, 2010, and Dec 24, 2014, 19 114 community-dwelling people in Australia and the USA, aged predominantly 70 years and older, were randomly assigned to low-dose aspirin or placebo for a median of 4·7 years as part of the ASPREE trial. Post-trial observational follow-up continued for a median of 4·3 years (IQR 4·1-4·6). All components of the primary endpoint (ie, incident dementia, persistent physical disability, and death) were adjudicated by masked expert panels. Analyses used Cox proportional hazards models with intention-to-treat.
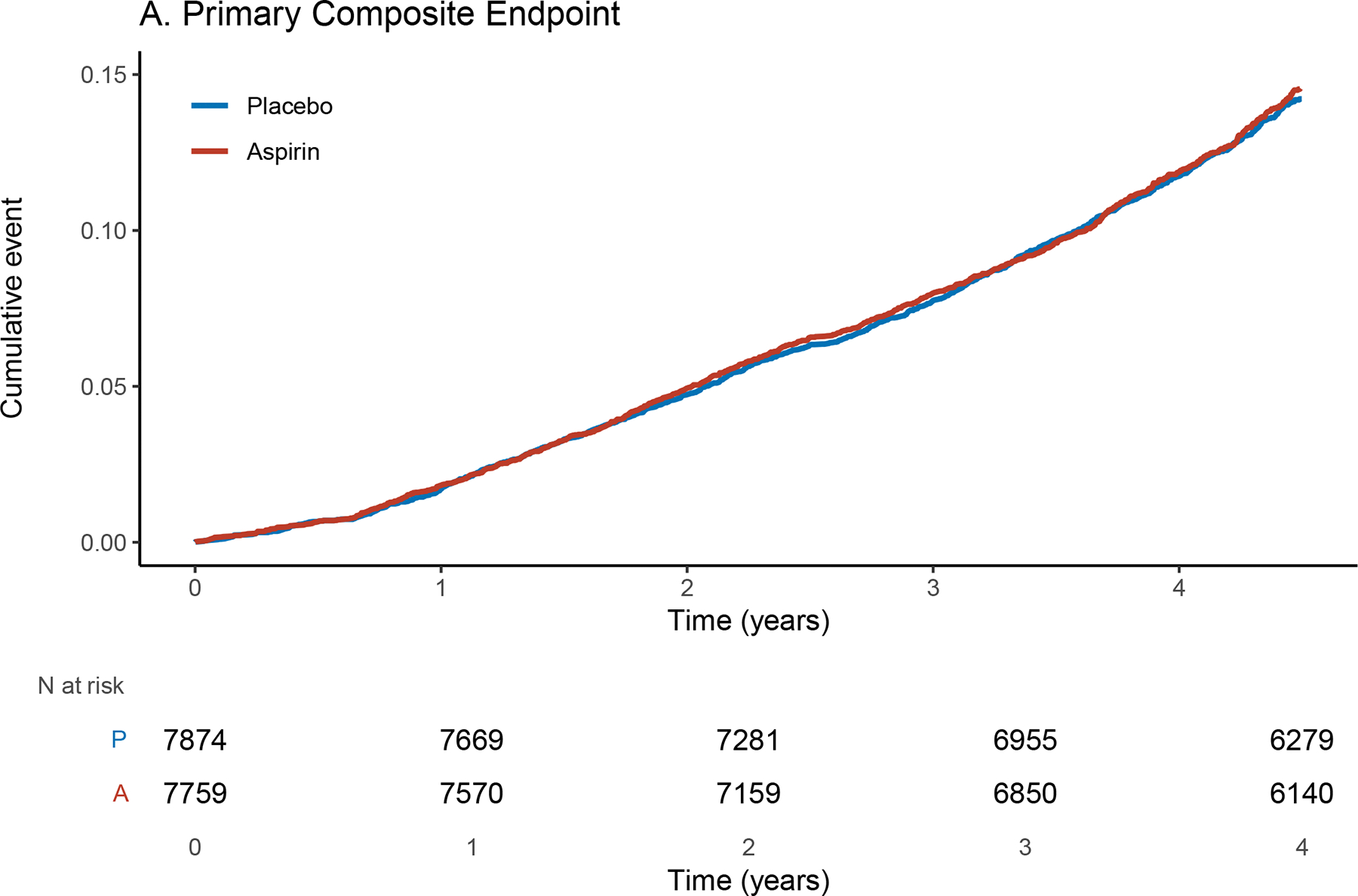
Findings: 15 633 participants (8836 [56·5%] were women, 6797 [43·5%] were men; 981 [6·3%] were not White) were eligible for and agreed to observational follow-up. There was no effect of randomisation to aspirin (34·37 events per 1000 person-years) versus placebo (33·68 per 1000 person-years) on the primary endpoint (hazard ratio [HR] 1·02; 95% CI 0·94-1·11; p=0·63) in the ASPREE-XT period. Similarly, over the period of both ASPREE and ASPREE-XT, no long-term effect of aspirin versus placebo was observed on the composite outcome of death, dementia, or persistent physical disability over almost a decade of follow-up (HR 1·01; 95% CI 0·95-1·08; p=0·65), including no long-term effect on deaths (1·06; 0·99-1·14; p=0·10). No effect of aspirin on incident major haemorrhagic events as compared with placebo was found in ASPREE-XT; however, aspirin was associated with an increased hazard for incident major haemorrhagic events across both ASPREE and ASPREE-XT (1·24; 1·10-1·39).
Interpretation: Low-dose aspirin does not appear to be effective in promoting a healthy lifespan in initially healthy, community-dwelling older people.
Funding: National Institute on Aging and the National Cancer Institute (USA).
Copyright © 2025 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests RCS reports grant funding for work as a clinical trial sub-investigator from Athira Pharma, Edgewater NEXT, Eisai, Eli Lilly, and Genentech, paid to his institution outside the submitted work. JR reports receiving grants from the National Institute on Aging outside of the submitted work. AC reports a consulting role for Pfizer and Boehringer Ingelheim and grant funding, paid to his institution, from Freenome outside the submitted work. TT-JC reports receiving honoraria for lectures from Roche outside the submitted work. SEE reports receiving grants from the National Institute on Aging and speaking honoraria from Yale University (New Haven, CT, USA), and the University of Rochester (Rochester, NY, USA) outside the submitted work. MRN reports receiving speaking fees from Medtronics outside of the submitted work. KS reports receiving grants from the National Institute on Aging along with the Agency for Health Care Research and Quality and writing honoraria from the International Antiviral Society USA outside of the submitted work. All other authors declare no competing interests.
Figures

References
-
- World Health Organization (WHO). Decade of healthy ageing: baseline report: summary. 2021. Accessed January 27, 2025. https://iris.who.int/bitstream/handle/10665/341488/9789240023307-eng.pdf
-
- Global Health Observatory. World Health Organization. Updated May 2024. Accessed January 27, 2025. https://www.who.int/data/gho/data/themes/mortality-and-global-health-est...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
