

Clinical psychopathology-based early relapse prediction model using speech and language in psychosis
- PMID: 41050346
- PMCID: PMC12493218
- DOI: 10.1016/j.scog.2025.100392
Clinical psychopathology-based early relapse prediction model using speech and language in psychosis
Abstract
Introduction: Prediction of psychotic relapse using speech-derived markers promises targeted early intervention. However, the sheer number of speech markers and the 'black box' nature of predictive models challenges clinical translation.
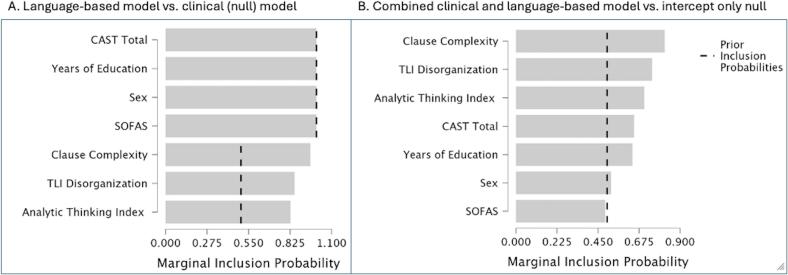
Methods: We propose a psychopathology-based systematic approach to identify likely relapse. We draw on the notion that the predictors of relapse should mark (1) the presence of schizophrenia in its untreated early stages and (2) track disorganization in psychosis. By leveraging Natural Language Processing, we derive 3 lexical, syntactic and narrative markers -semantic similarity, clause complexity, and analytic thinking index from speech samples of people with acute psychosis (n = 68) followed up for subsequent relapses over a year (12 out of 68).
Results: Speech-based model predicted relapse status with strong evidence (Bayes Factor BF10 = 79.5) against the clinical intuition model.
Conclusion: Using a Bayesian approach, this preliminary study demonstrates the utility of psychopathology-guided variable selection for speech-based relapse prediction complementing clinical intuition in practice.
Keywords: Computational linguistics; Disorganization; Early intervention; Impoverishment; Precision psychiatry; Relapse; Thought disorder.
© 2025 The Authors. Published by Elsevier Inc.
Conflict of interest statement
LP reports personal fees for serving as chief editor from the Canadian Medical Association Journals, speaker/consultant fee from Janssen Canada and Otsuka Canada, SPMM Course Limited, UK, Canadian Psychiatric Association; book royalties from Oxford University Press; investigator-initiated educational grants from Janssen Canada, Sunovion and Otsuka Canada outside the submitted work. All other authors report no potential conflicts.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
