

Tidal volume and mortality during extracorporeal membrane oxygenation for acute respiratory distress syndrome: a multicenter observational cohort study
- PMID: 41051703
- PMCID: PMC12500509
- DOI: 10.1186/s13613-025-01538-9
Tidal volume and mortality during extracorporeal membrane oxygenation for acute respiratory distress syndrome: a multicenter observational cohort study
Abstract
Background: Approximately half of the patients with acute respiratory distress syndrome (ARDS) receiving extracorporeal membrane oxygenation (ECMO) remain ECMO-dependent beyond 14 days after ECMO initiation. The identification of factors associated with mortality during an ECMO run may update prognostic assessment and focus clinical interventions.
Methods: In this observational study, data from 1137 patients with COVID-19 ARDS receiving ECMO support in 29 German centers between January 1st 2020 and July 31st 2021 were analyzed. Multivariable stepwise logistic regression analyses were performed to build survival prediction models with day-by-day data during the first 14 days of an ECMO run. The primary endpoint was all-cause mortality in the intensive care unit.
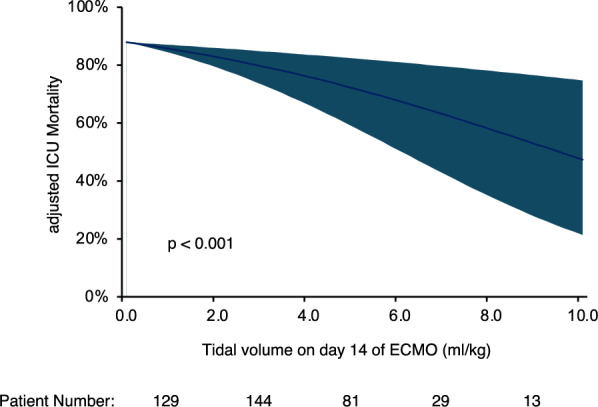
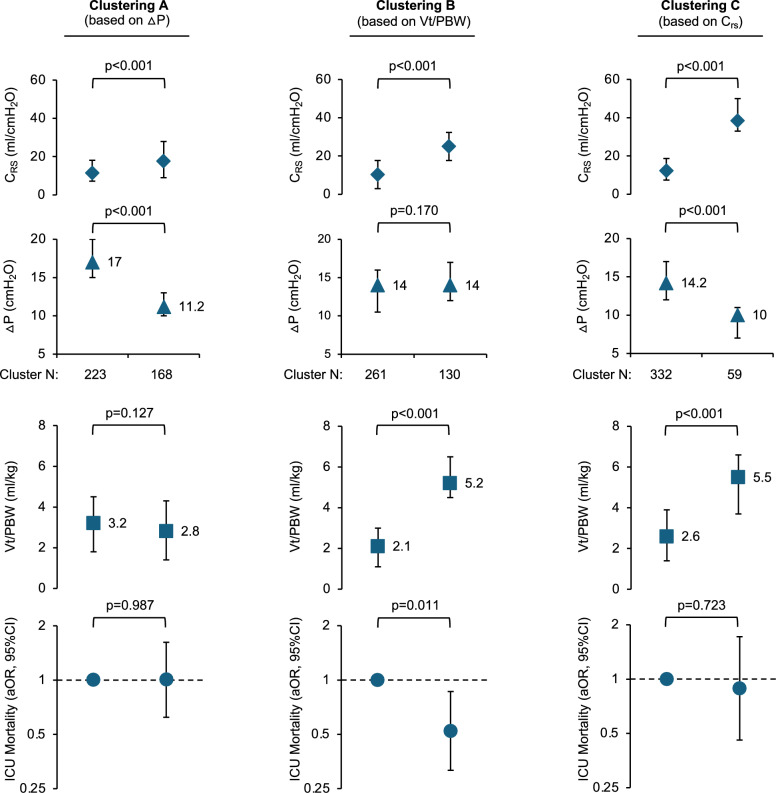
Results: Mortality in this cohort was high (75%). Patients who remained ECMO-dependent on day 14 of their ECMO run showed comparable mortality to all patients receiving ECMO support on day 1. Yet, factors associated with mortality changed during the first 14 days of ECMO support. On day 1 of ECMO support, only patient age and lactate remained in the final mortality prediction model. On day 14 of an ECMO run, tidal volume was independently associated with mortality (adjusted Odds Ratio 0.693 (95%CI 0.564-0.851), p < 0.001 for 1 mL/kg increase in tidal volume per predicted body weight). The adjusted mortality for patients with a tidal volume below 2 mL/kg on day 14 of their ECMO run was above 80% (lower limit of the 95%CI interval). Higher tidal volume was mainly based on higher respiratory system compliance. Yet, the benefit of higher compliance was not observed in some patients who were still ventilated with very low driving pressures despite remaining ECMO-dependent on day 14 of ECMO support.
Conclusions: Mortality predictors change during the course of an ECMO run. In a cohort with high mortality, on day 14 of ECMO support for ARDS, tidal volume may be an independent predictor of mortality. Further analyses on ventilation strategies in patients who remain ECMO-dependent are needed.
Trial registration number: DRKS00022964, retrospectively registered.
Keywords: ARDS; ECMO; Mortality prediction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol for the German COVID-19 ECMO registry was approved by the Ethics Committee of the Medical Faculty of the Julius-Maximilians-University of Würzburg (131/20-me). Additional local ethics committee votes were obtained from each of the participating ECMO centers. The analysis of data derived from patients treated at the Saarland University Medical Center was approved by the local ethics committee (Landesärztekammer des Saarlandes, 59/24). According to German legislation, no informed consent for retrospective, anonymous data is required and informed consent was waived by the ethics committee. Consent for publication: Not applicable. Competing interests: All authors declare no competing interests.
Figures

References
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374:1351–63. - DOI - PubMed
LinkOut - more resources
Full Text Sources
