

Cost-effectiveness of respiratory syncytial virus prevention strategies in Mozambique: a modelling study
- PMID: 41059446
- PMCID: PMC12499514
- DOI: 10.7189/001c.137870
Cost-effectiveness of respiratory syncytial virus prevention strategies in Mozambique: a modelling study
Abstract
Background: Respiratory syncytial virus (RSV) is a leading cause of severe acute lower respiratory infections in children. The World Health Organization recently recommended two passive RSV immunisation strategies for global use, but prices are yet to be determined in low- and middle-income countries (LMICs).
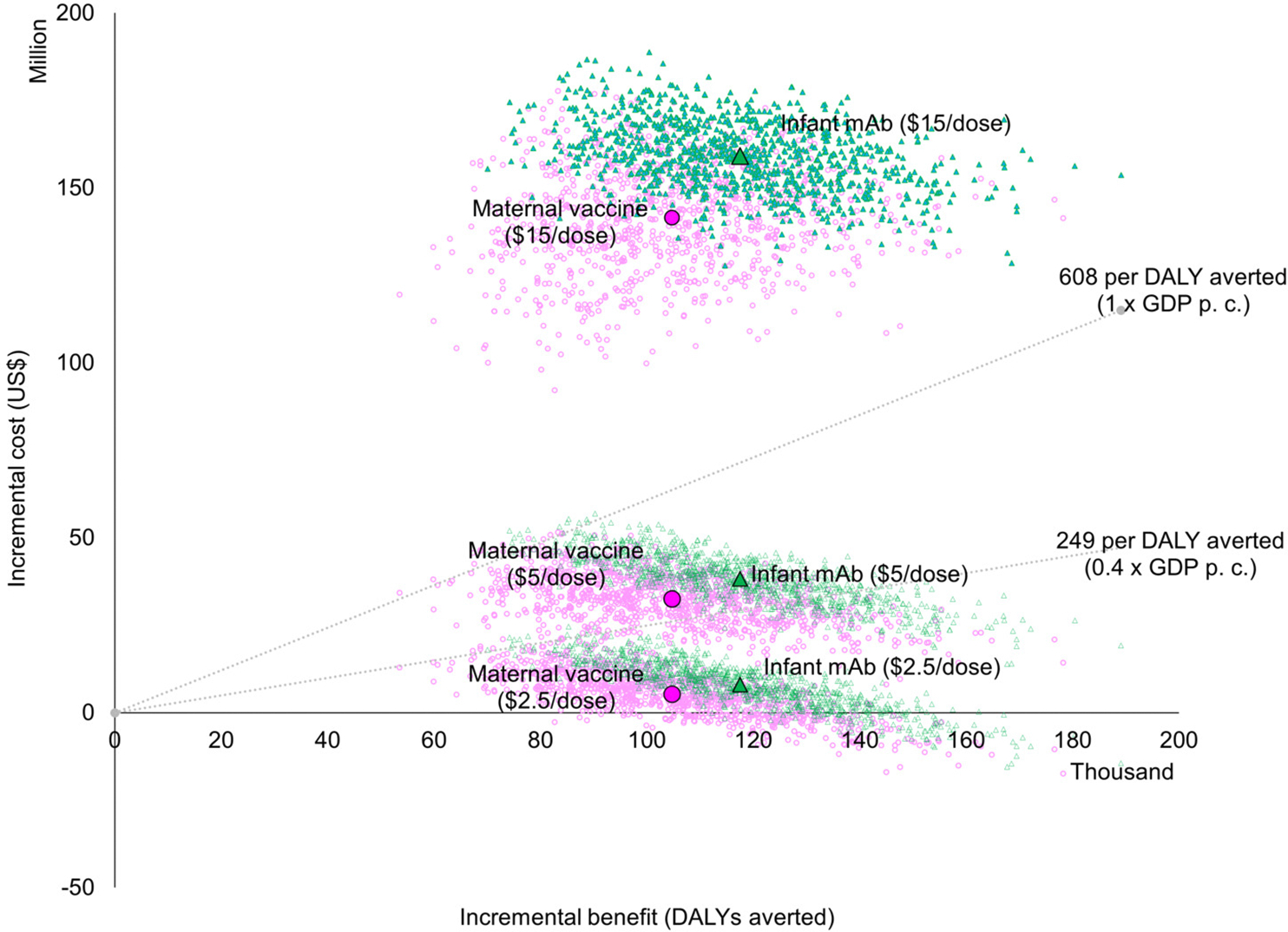
Methods: We used a static cohort model to generate preliminary estimates of the potential health impact and cost-effectiveness of a maternal vaccine (RSVPreF, Abrysvo®, Pfizer) and a long-acting infant mAb (Nirsevimab, Beyfortus®, AstraZeneca, and Sanofi) over a 10-year period (2025-2034) in Mozambique. We incorporated cost-of-illness data from a recent study conducted in Maputo, Mozambique, and efficacy data from recent clinical trials. We compared each RSV prevention strategy to the current status quo (no pharmaceutical RSV prevention strategy). The primary outcome was the cost per disability-adjusted life year (DALY) averted from a government perspective, assuming year-round dose administration. We ran a range of deterministic scenarios, including a societal health perspective and a seasonal dose administration strategy. We also ran probabilistic uncertainty analyses and estimated the probability that each intervention would be cost-effective over a range of cost-effectiveness thresholds.
Results: Year-round administration of a maternal vaccine (USD 5/dose, 69% efficacy, 87% coverage, 6 months protection) could cost USD 80 million and prevent 4,671 RSV deaths. Year-round administration of the long-acting infant mAb (USD 5/dose, 77% efficacy, 94% coverage, 5 months protection) could cost USD 85 million and prevent 5,128 RSV deaths. Over half the cost of the respective programs would be offset by healthcare cost savings. Compared to the current status quo, the cost per DALY averted from a government perspective was USD 288 (95% uncertainty interval 140-574) for the maternal vaccine and USD 289 (95% uncertainty interval 160-583) for the mAb. At an intervention price of USD 5 per dose, the probability is around 20% that either intervention is cost-effective at a threshold of 0.4 times the national GDP per capita.
Conclusions: New passive immunisation interventions have the potential to prevent a substantial number of infant deaths in Mozambique. Both interventions have the potential to be cost-effective if priced below USD 5 per dose. A seasonal strategy could further improve cost-effectiveness if feasible to implement.
Keywords: RSV; cost-effectiveness analysis; low-income country; maternal vaccine; monoclonal antibody.
Conflict of interest statement
DISCLOSURE OF INTEREST The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Figures

References
-
- WHO. Respiratory Syncytial Virus (RSV) disease. 2023. Accessed August 16, 2023. https://www.who.int/teams/health-product-policy-and-standards/standards-...
-
- Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. The Lancet. 2022;399(10340):2047–2064. Accessed August 15, 2023. https://linkinghub.elsevier.com/retrieve/pii/S0140673622004780
-
- UN IGME UI agency G for CME. Mozambique: Under-five mortality rate - Total. 2023. Accessed August 28, 2024. https://childmortality.org/all-cause-mortality/data/estimates?indicator=...
-
- Pale M, Tivane A, Gilds T, Bauhofer A, Nguenha N, Machalele L, et al. Risk factors and circulation pattern of respiratory syncytial virus in children under 2 years in Maputo, Mozambique. Int Health. 2024;0:1–9. Accessed September 10, 2024. https://pubmed.ncbi.nlm.nih.gov/38717389/
-
- Abdelrahman DN, Abdullahi FL, Abdu-Raheem F, Abicher LT, Adelaiye H, Badjie A, et al. Respiratory syncytial virus infection among children younger than 2 years admitted to a paediatric intensive care unit with extended severe acute respiratory infection in ten Gavi-eligible countries: the RSV GOLD—ICU Network study. The Lancet Global Health. 2024;12(10):E1611–E1219. doi: 10.1016/S2214-109X(24)00269-9 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous