

The prognostic importance of left ventricular diastolic function in primary mitral regurgitation and its relation to structural changes by CMR
- PMID: 41062547
- PMCID: PMC12508152
- DOI: 10.1038/s41598-025-18965-0
The prognostic importance of left ventricular diastolic function in primary mitral regurgitation and its relation to structural changes by CMR
Abstract
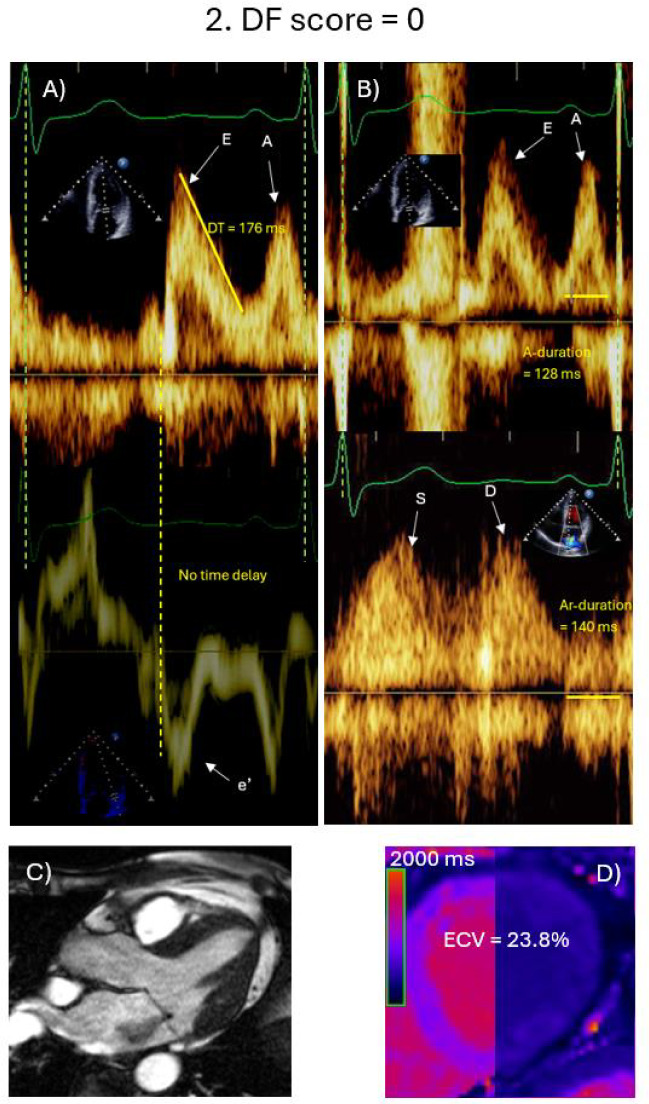
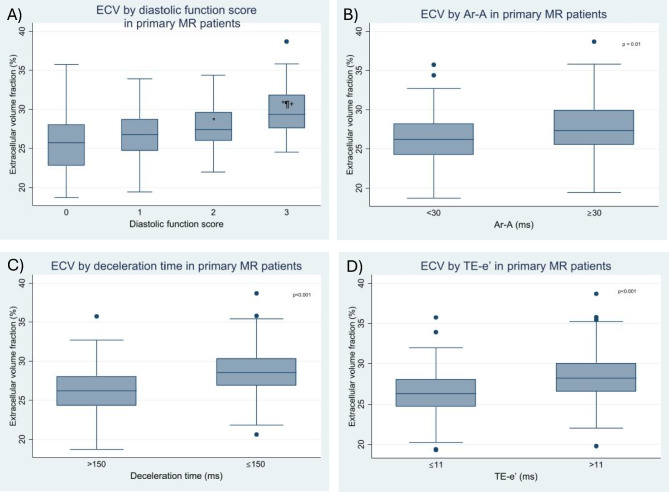
Patients with significant primary mitral regurgitation (MR) can develop left ventricular (LV) diastolic dysfunction (DD). We sought to study LV structural correlates, and prognostic significance of DD. Patients with ≥ moderate primary MR with echocardiographic and CMR scans within a median time of 5 days were included. LV volumes, EF, MR volume and fraction, presence of scar, and extracellular volume (ECV) were assessed by CMR. LV diastolic function (DF) was assessed by echocardiography using time delay between onset of mitral E velocity and mitral annulus e' velocity, deceleration time of mitral E velocity, and duration difference between pulmonary vein atrial velocity and mitral A velocity. DF score was computed based on these 3 variables. Event rate (heart failure hospitalizations, cardiovascular death, or mitral valve surgery) was higher in patients with DD versus patients with normal DF (P < 0.05). MR volumes, and ECV were significantly higher in patients with DD (P < 0.001). In multivariable cox proportional hazard model, inclusion of DF score increased AUC from 0.83 to 0.86. Thus, DD is associated with ECV, MR severity, and clinical outcomes. DD score provides incremental value for the prediction of adverse outcomes when added to clinical characteristics, MR severity, and LV end diastolic volume index.
Keywords: Diastolic function; Left ventricle; Mitral regurgitation; Outcome.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures


References
-
- Avierinos, J.-F. et al. Natural history of asymptomatic mitral valve prolapse in the community. Circulation106, 1355–1361 (2002). - PubMed
-
- Enriquez-Sarano, M., Akins, C. W. & Vahanian, A. Mitral regurgitation. Lancet373, 1382–1394 (2009). - PubMed
-
- Bakkestrøm, R. et al. Hemodynamic characteristics in significant symptomatic and asymptomatic primary mitral valve regurgitation at rest and during exercise. Circ Cardiovasc Imaging11, e007171 (2018). - PubMed
-
- Edwards, N. C. et al. Quantification of left ventricular interstitial fibrosis in asymptomatic chronic primary degenerative mitral regurgitation. Circ. Cardiovasc. Imaging7, 946–953 (2014). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
