

Primary age-related tauopathy
- PMID: 41065841
- PMCID: PMC12511220
- DOI: 10.1007/s00401-025-02943-x
Primary age-related tauopathy
Abstract
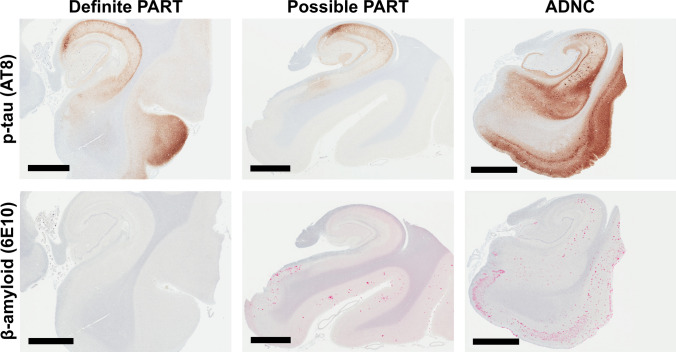
Primary age-related tauopathy (PART) was proposed in 2014 as a neuropathological term to describe patients with Alzheimer's-type medial temporal lobe neurofibrillary degeneration in the absence of significant β-amyloid pathology. Over the past decade, this designation has gained widespread adoption, helping to clarify the interpretation of biomarker profiles, delineate early-stage tauopathy in aging, and differentiate non-Alzheimer tauopathies from aging and classical Alzheimer disease. This review revisits PART ten years following its conception, critically evaluating its neuropathological features, clinical correlates, molecular underpinnings, and current limitations. We synthesize recent advances in neuroimaging, biomarkers, genetics, and epidemiology, explore the relationship between PART and other age-associated neurodegenerative processes, and propose revisions to the original PART criteria. While PART has served as a valuable framework for studying tau pathology in aging, key questions remain regarding its pathogenesis, clinical significance, and relationship to the broader spectrum of tauopathies. We highlight major gaps in knowledge and outline priorities for future research aimed at defining the mechanisms, biomarkers, and clinical criteria that will determine whether PART represents a distinct disease or a universal feature of human brain aging.
Keywords: Aging; Alzheimer’s disease neuropathologic change (ADNC); CA1 hippocampal subfield; Cognitive reserve; Cornu ammonis 2 (CA2) hippocampal subfield; Limbic-predominant age-related TDP-43 encephalopathy neuropathologic change (LATE-NC); Primary age-related tauopathy (PART); Resilience.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: T.E.R. has been a consultant for Servier Pharmaceuticals. T.G.O. has been a consultant for Sonae and Guidepoint and has received speaker fees from Eisai and conference fees covered from Roche and Lilly. The authors declare that these disclosures are unrelated to the present work, and that they have no additional competing interests, conflicts of interest, or other relevant disclosures. Ethical approval and consent to participate: Not applicable. Consent for publication: Not applicable.
Figures




References
-
- Agrawal S, Yu L, Barnes LL, Bennett DA, Boyle PA, Schneider JA (2025) Cognitive decline in community-dwelling older persons with primary age-related tauopathy: role of anatomical location of tangles and other co-existing brain pathologies. Acta Neuropathol 150:8. 10.1007/s00401-025-02916-0 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P20 AG068053/AG/NIA NIH HHS/United States
- P30 AG066515/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- P30 AG066508/AG/NIA NIH HHS/United States
- P30 AG066519/AG/NIA NIH HHS/United States
- P30 AG072973/AG/NIA NIH HHS/United States
- P30 AG066462/AG/NIA NIH HHS/United States
- P30 AG066530/AG/NIA NIH HHS/United States
- P30 AG066509/AG/NIA NIH HHS/United States
- P20 AG068077/AG/NIA NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- P30 AG072972/AG/NIA NIH HHS/United States
- P30 AG072979/AG/NIA NIH HHS/United States
- P20 AG068082/AG/NIA NIH HHS/United States
- P30 AG072975/AG/NIA NIH HHS/United States
- P30 AG066444/AG/NIA NIH HHS/United States
- P30 AG066507/AG/NIA NIH HHS/United States
- P30 AG072946/AG/NIA NIH HHS/United States
- P30 AG066518/AG/NIA NIH HHS/United States
- P30 AG066511/AG/NIA NIH HHS/United States
- U24 AG072122/AG/NIA NIH HHS/United States
- P30 AG066512/AG/NIA NIH HHS/United States
- P30 AG072978/AG/NIA NIH HHS/United States
- P30 AG062429/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- R01 AG079280/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- P30 AG062677/AG/NIA NIH HHS/United States
- P20 AG068024/AG/NIA NIH HHS/United States
- P30 AG072958/AG/NIA NIH HHS/United States
- P30 AG062715/AG/NIA NIH HHS/United States
- P30 AG066506/AG/NIA NIH HHS/United States
- P30 AG066468/AG/NIA NIH HHS/United States
- P30 AG072976/AG/NIA NIH HHS/United States
- P30 AG072947/AG/NIA NIH HHS/United States
- P30 AG072931/AG/NIA NIH HHS/United States
- P30 AG066514/AG/NIA NIH HHS/United States
- P30 AG072959/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
