

Bipolar hemiarthroplasty for femoral neck fractures in elderly patients: a retrospective study of 1001 patients
- PMID: 41081918
- PMCID: PMC12518434
- DOI: 10.1007/s00402-025-06073-7
Bipolar hemiarthroplasty for femoral neck fractures in elderly patients: a retrospective study of 1001 patients
Abstract
Introduction: Displaced intracapsular femoral neck fractures (FNF) are the most frequent surgical pathology in orthopedics. Controversy surrounds optimal treatment, with little consensus, particularly in the elderly multimorbid at risk population. For over a decade, our institution adopts a standardized protocol for FNF, utilizing cemented hip hemiarthroplasty (HA) via the posterior approach. This study evaluates the outcomes of this approach, contributing to the ongoing debate and potentially guiding future treatment strategies.
Methodology: This retrospective study included patients (≥ 60 years) who underwent HA for FNF from January 1, 2008, to June 30, 2019, at a University Hospital. Our primary endpoint was revision surgery for HA (rHA) within four years after HA. Secondary endpoints included hip-related and unrelated complications.
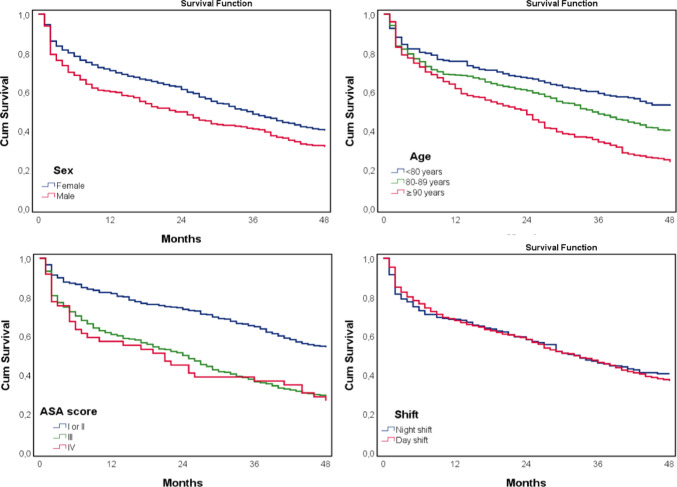
Results: Of 1001 patients, 40 (3.9%) underwent rHA. Indications were periprosthetic fractures (5; 0.5%), dislocation (15; 1.5%), suspected prosthetic joint infection (17; 1.7%), and acetabular erosion (3; 0.3%). Four-year mortality was 51%. Cox regression revealed age > 80 years (aHR 1.86, p < 0.001), ASA score III or IV (aHR 2.11, p < 0.001), and postoperative delirium (aHR 1.29, p < 0.05), as independent predictors of higher 4-year mortality. No difference was observed among patients with and without revision indication for ASA scores III or IV (64% vs. 64%; p = 0.912), surgery within 24 h (52% vs. 57%; p = 0.334), duration over 90 min (46% vs. 53%; p = 0.201), and surgery during the night shift (24% vs. 19%; p = 0.285). Board certification did not impact revision rates (39% vs. 39%; p = 1.000).
Conclusion: Cemented HA is a safe and reliable treatment option for FNF, delivering consistent outcomes in the elderly multimorbid population, with low rates of rHA (3.9%). The posterior surgical approach, even in patients with heightened dislocation risk, remains a viable option. Timing of surgery (night/day) does not significantly affect revision rates, which could have substantial implications for surgical planning and healthcare resource allocation.
Keywords: Acetabular erosion; Bipolar hemiarthroplasty; Dislocation; Femoral neck fractures; Geriatric orthopedics; Prosthetic joint infection.
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests.
Figures


References
-
- SIRIS. https://www.swiss-medtech.ch/sites/default/files/2023-11/231117_SIRIS-Re.... Accessed 4 Aug 2024
-
- Williamson S, Landeiro F, McConnell T et al (2017) Costs of fragility hip fractures globally: a systematic review and meta-regression analysis. Osteoporos Int 28:2791–2800. 10.1007/s00198-017-4153-6 - PubMed
-
- Healy WL, Iorio R (2004) Total hip arthroplasty: optimal treatment for displaced femoral neck fractures in elderly patients. Clin Orthop 429:43–48. 10.1097/01.blo.0000150273.13949.62 - PubMed
-
- Ravi B, Pincus D, Khan H (2019) Comparing complications and costs of total hip arthroplasty and hemiarthroplasty for femoral neck fractures: a propensity score-matched, population-based study. J Bone Joint Surg 101:572–579. 10.2106/JBJS.18.00539 - PubMed
LinkOut - more resources
Full Text Sources
