

Dual doppler dynamics: integrating femoral venous doppler and VExUS for predicting organ dysfunction in acute heart failure
- PMID: 41094573
- PMCID: PMC12522689
- DOI: 10.1186/s44158-025-00283-6
Dual doppler dynamics: integrating femoral venous doppler and VExUS for predicting organ dysfunction in acute heart failure
Abstract
Background: Heart failure (HF) leads to venous congestion (VC), leading to organ dysfunction. Traditional VC assessments include pulmonary artery catheterization and IVC ultrasound. Newer tools like venous excess ultrasound (VExUS) and femoral venous doppler (FVD) quantify VC severity. We aimed to compare FVD with VExUS score to predict organ dysfunction and its progression in acute HF patients.
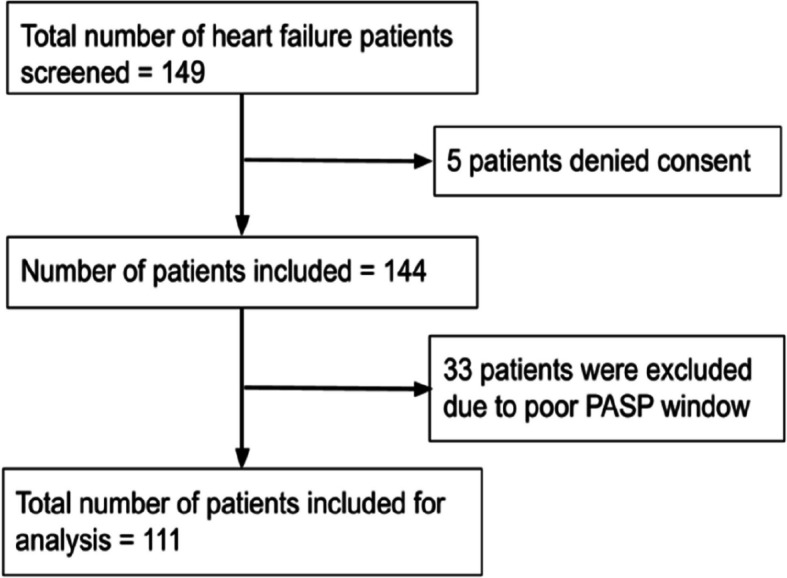
Methods: We conducted a 6-month prospective study in a 36-bed Cardiac ICU, enrolling 111 adults with acute decompensated HF. We evaluated FVD and VExUS to predict organ dysfunction and its progression. Key parameters were recorded on ICU admission and Day 3. We followed up patients at 90-days using the MAKE-90 criteria. Sensitivity, specificity, and predictive values of FVD and VExUS were calculated and compared using McNemar's test.
Results: VC was higher in the organ dysfunction group, with higher VExUS scores (55% vs. 31%, p = 0.018) and FVD-defined congestion (85% vs. 57%, p = 0.002). This group also revealed worse LUS, lower TAPSE:PASP ratios, more severe AKI, higher creatinine, and increased use of non-invasive ventilation (all p < 0.01). Mortality (39% vs. 24%) and MAKE-90 events (56% vs. 39%) were higher but not statistically significant. FVD had higher sensitivity but lower specificity than VExUS in detecting AKI, and lung congestion. VExUS had higher specificity for RV coupling and organ dysfunction; FVD correlated more with organ dysfunction.
Conclusion: FVD and VExUS provide complementary insights into venous congestion, reinforcing the need for an integrated approach rather than reliance on a single modality. A multimodal strategy combining these tools with clinical and biochemical markers may offer a more precise framework for guiding management in acute heart failure.
Trial registration: This trial was registered with Clinical Trial Registry-India ( https://www.ctri.nic.in/ ), Trial No-CTRI/2023/10/058186 on 3/10/2023.
Keywords: Acute kidney injury; Femoral venous doppler; Organ dysfunction; Venous congestion; Venous excess ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Narayana Health Academic Ethics Committee (Approval #NHH/AEC-CL-2023–1008; August 2023) approved the conduct of this study. This trial was registered with Clinical Trial Registry-India ( https://www.ctri.nic.in/ ), Trial Number—CTRI/2023/10/058186 on 3/10/2023. Informed consent from the patient was obtained before the screening process. Patients who declined consent were not included in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
References
-
- ICC-NHFR [Internet]. Available from: https://www.iccnhfr.org/. Cited 2025 Apr 6
-
- Rosenkranz S, Howard LS, Gomberg-Maitland M, Hoeper MM (2020) Systemic consequences of pulmonary hypertension and right-sided heart failure. Circulation 141(8):678–693 - PubMed
-
- Pinsky MR (2012) Pulmonary artery occlusion pressure. In: Pinsky MR, Brochard L, Hedenstierna G, Antonelli M, editors. Applied Physiology in Intensive Care Medicine 1: Physiological Notes-Technical Notes-Seminal Studies in Intensive Care [Internet]. Berlin, Heidelberg: Springer. p 83–6. Available from: 10.1007/978-3-642-28270-6_19. Cited 2025 May 18 - DOI
-
- Longino AA, Martin KC, Douglas IS (2024) Monitoring the venous circulation: novel techniques and applications. Curr Opin Crit Care 30(3):260–267 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous