

Incidence and outcomes of extubation failure in mechanically ventilated patients with cirrhosis: a post-hoc analysis of a prospective multicenter study
- PMID: 41099917
- PMCID: PMC12532547
- DOI: 10.1186/s13613-025-01576-3
Incidence and outcomes of extubation failure in mechanically ventilated patients with cirrhosis: a post-hoc analysis of a prospective multicenter study
Abstract
Background: Patients with comorbidities who are liberated from invasive mechanical ventilation could be at risk of extubation failure in the intensive care unit (ICU). Incidence and associated outcomes of reintubation in patients with cirrhosis have been poorly studied. We aimed to evaluate the incidence, causes and mortality of reintubation in patients with cirrhosis.
Methods: We conducted a post hoc analysis of the French prospective multicenter observational trial (FREE-REA) evaluating the incidence and risk factors of extubation failure in 26 ICUs. The primary outcome was the incidence of extubation failure defined as the need for reintubation within 7 days after extubation. Secondary outcomes were the incidence of reintubation at 48 h, the causes and risk factors of extubation failure, ICU length of stay and in-hospital mortality. We compared patients with cirrhosis and patients without cirrhosis.
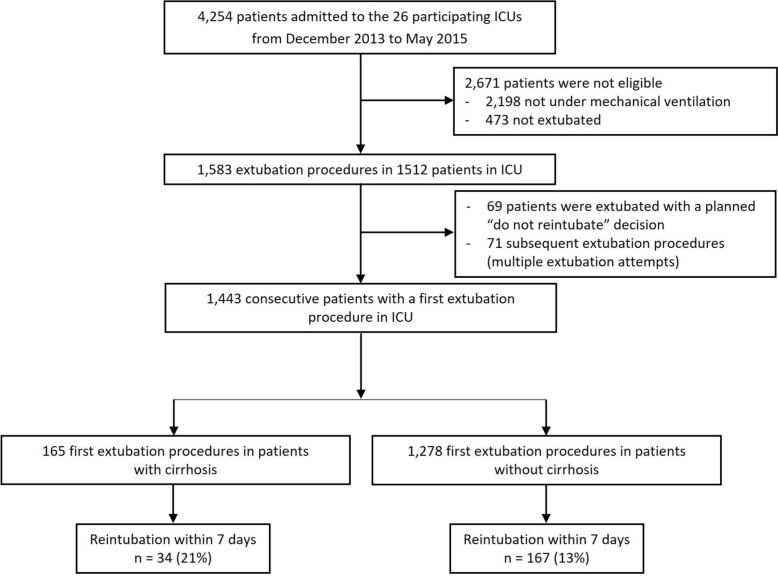
Results: Of the 1,443 analyzed patients, 165 (11%) had cirrhosis. The incidence of reintubation within 7 days was 21% (34/165) in patients with cirrhosis and 13% (167/1278) in patients without cirrhosis (p < 0.01). Reintubation at 48 h was not significantly different between patients with cirrhosis and patients without cirrhosis (9% versus 10%, p = 0.55). Admission for shock was identified as the only independent risk factor for extubation failure in multivariate analysis [OR 3.24, 95% CI (1.24-8.44), p = 0.02]. In patients with extubation failure, ICU length of stay was significantly longer in patients with cirrhosis compared to those without (28 ± 25 versus 18 ± 12 days, p < 0.01); In-hospital mortality was higher in extubation failure patients with cirrhosis in comparison to patients without cirrhosis without reaching significance (16/34 (47%) versus 51/167 (31%), p = 0.06).
Conclusion: Extubation failure was significantly higher in patients with cirrhosis compared to patients without cirrhosis. A trend for higher in-hospital mortality was observed in reintubatedpatients with cirrhosis. Neurologic failure was the main cause for reintubation at 48 h in patients with cirrhosis.
Clinical trials: The study was registered on clinicaltrials.gov (identifier no. NCT02450669). Registered 01/12/2013.
Keywords: Cirrhosis; Extubation failure; Intensive care unit; Mechanical ventilation.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The appropriate IRB (Comité de Protection des personnes Sud-Mediterranée III) approved the study protocol (code UF: 9242, register: 2013-A01402–43)., and, based on the observational design, waived the need for written informed consent. Next of kin were informed of the study, as were patients as soon as their neurologic status was deemed adequate. Written information was delivered to the patient’s next of kin and to the patient when neurologic recovery was deemed appropriate. The study was registered on ClinicalTrials.gov (identifier number NCT 02450669). Consent for publication: Not applicable. Competing interests: Pr. Jaber reports receiving consulting fees from Drager, Medtronic, Baxter, Fresenius-Xenios, Mindray, and Fisher & Paykel. Dr. De Jong reports receiving consulting fees from Medtronic, Dräger, Viatris and Fisher & Paykel. No conflict of interests is reported for other authors.
Figures

References
-
- Ginès P, Krag A, Abraldes JG, Solà E, Fabrellas N, Kamath PS. Liver cirrhosis. Lancet. 2021;398:1359–76. - PubMed
-
- Lee KC, Chiang AA. The outcome of terminal liver cirrhosis patients requiring mechanical ventilation. Zhonghua Yi Xue Za Zhi Chin Med J Free China Ed. 1997;59:88–94. - PubMed
-
- Levesque E, Saliba F, Ichaï P, Samuel D. Outcome of patients with cirrhosis requiring mechanical ventilation in ICU. J Hepatol. 2014;60:570–8. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
