

Evaluating the effectiveness of thoracoscopic intervention for pulmonary abscess: is lobectomy the optimal solution after medical therapy fails?
- PMID: 41107810
- PMCID: PMC12534970
- DOI: 10.1186/s12893-025-03167-2
Evaluating the effectiveness of thoracoscopic intervention for pulmonary abscess: is lobectomy the optimal solution after medical therapy fails?
Abstract
Background: Lung abscess is typically managed by performing abscess drainage. While pulmonary resection effectively controls infection, its role in eliminating necrotic tissue remains debatable due to risks such as bleeding, desaturation, systemic inflammation, persistent air leakage, and bronchopleural fistula. In this study, we evaluated the outcomes of pulmonary resection for lung abscess refractory to medical therapy.
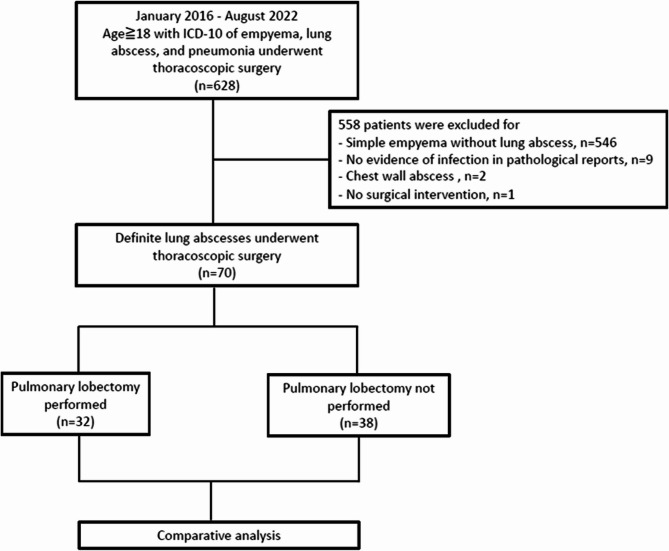
Methods: We retrospectively analyzed 70 patients who underwent salvage thoracoscopic surgery for lung abscess, along with 60 days' follow-up, at a tertiary referral hospital between January 2016 and August 2022. Thirty-two patients underwent lobectomy, while 38 did not. The patients' demographics, comorbidities, disease progression, 30-day and 60-day mortality, and operative morbidity were compared between the lobectomy and non-lobectomy groups.
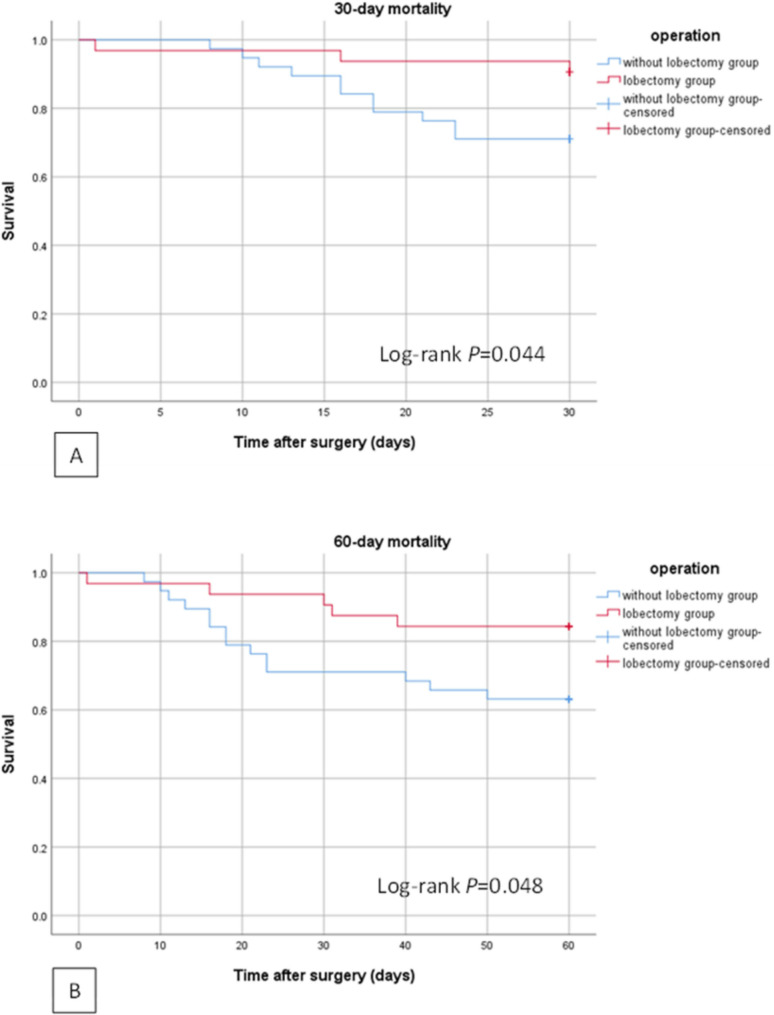
Results: Necrotizing pneumonia was the leading cause of lung abscess (n = 53, 75.7%), with empyema being the most common sign of disease progression (n = 36, 51.4%). The lobectomy group had a lower mortality rate compared with the non-lobectomy group (15.6% vs. 36.8%, p = 0.047). Multivariate analysis identified a higher Charlson Comorbidity Index (CCI) as a risk factor for 30-day mortality (HR = 1.286, 95% CI = 1.059-1.561; p = 0.011), while lobectomy mitigated the 30-day mortality risk (HR = 0.255, 95% CI = 0.068-0.959; p = 0.043). Similarly, a higher CCI augmented the 60-day mortality risk (HR = 1.317, 95% CI = 1.105-1.571; p = 0.002), whereas lobectomy lowered it (HR = 0.319, 95% CI = 0.110-0.921; p = 0.035).
Conclusion: Lobectomy significantly improves the 30- and 60-day mortality outcomes compared to non-lobectomy surgery, making it a viable option for pharmacotherapy-refractory lung abscess.
Keywords: Lobectomy; Lung abscess; Mortality; Pulmonary abscess drainage; Pulmonary resection.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. This study was initiated by the Far Eastern Memorial Hospital. The study was approved by the Institutional Review Board (IRB) of Far Eastern Memorial Hospital (IRB approval no. 111279-E), which waived the need for informed consent. Consent for publication: All authors in our study group agreed on the order of authorship and publication. Competing interests: The authors declare no competing interests.
Figures
References
-
- Zhang JH, Yang SM, How CH, Ciou YF. Surgical management of lung abscess: from open drainage to pulmonary resection. J Vis Surg. 2018;4:224. 10.21037/jovs.2018.10.14.
-
- Krishnadasan B, Sherbin VL, Vallières E, Karmy-Jones R. Surgical management of lung gangrene. Can Respir J. 2000;7:401–4. 10.1155/2000/174703. - PubMed
-
- Puligandla PS, Laberge JM. Respiratory infections: pneumonia, lung abscess, and empyema. Semin Pediatr Surg. 2008;17:42–52. 10.1053/j.sempedsurg.2007.10.007. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
